Opinion
Social and Biological Landscape of Kidney Disease in Sri Lanka
World Kidney Day falls today
The Chronic Kidney Disease (CKD) crisis in Sri Lanka represents one of the most formidable public health challenges of the twenty-first century, manifesting as a complex tapestry of environmental, social, and physiological factors. Unlike the traditional forms of kidney disease seen in urban centres—which typically stem from well-understood comorbidities like long-term diabetes and hypertension—the situation in the Sri Lankan ‘Dry Zone’ is defined by a mysterious and aggressive variant known as Chronic Kidney Disease of unknown aetiology (CKDu). This specific form of the disease has devastated the agricultural heartlands, particularly the North Central Province, for over three decades, yet it continues to evolve in its geographic reach and its socio-economic impact as of 2026. The persistence of this epidemic despite extensive international research highlights a profound gap in our understanding of how tropical environments and traditional occupational hazards intersect to damage human renal systems.
Historically, the emergence of CKDu was first noted in the late 1990s around the Anuradhapura and Polonnaruwa districts. What began as sporadic cases in rural hospitals quickly transformed into a localized epidemic, catching the medical community off guard because the patients did not present with the usual risk factors. These were not the sedentary, elderly populations usually associated with renal failure; rather, they were lean, active, middle-aged rice farmers.
The demographic specificity of the disease remains a chilling hallmark of the crisis today. It predominantly strikes men during their peak productive years, which triggers a catastrophic ripple effect through the family unit. When a primary breadwinner in a subsistence farming household falls ill, the family is thrust into a ‘poverty trap’ where limited resources are redirected toward transport to distant clinics, expensive nutritional supplements, and eventually, the gruelling routine of dialysis. This economic erosion often forces children out of school and into labour, perpetuating a cycle of systemic vulnerability that lasts for generations.
Intense scientific debate
The aetiology of the disease remains a subject of intense scientific debate and is currently viewed through a multifactorial lens. Researchers have moved away from the search for a single ‘smoking gun’ and are instead examining a lethal synergy of environmental triggers. Groundwater quality remains at the forefront of this investigation. The dry zone of Sri Lanka is characterized by high levels of fluoride and groundwater hardness, and it is theorized that the interaction between these natural minerals and anthropogenic pollutants—such as heavy metals from agrochemicals—creates a nephrotoxic cocktail.
The historical reliance on chemical fertilizers and pesticides in the ‘Green Revolution’ era of Sri Lankan agriculture is often cited as a major contributing factor. While direct links to specific brands of pesticides have been difficult to prove definitively, the accumulation of cadmium, arsenic, and lead in the soil and food chain continues to be monitored as a primary catalyst for the slow, progressive scarring of the kidney tubules.
In recent years, the discourse around CKDu has expanded to include the role of heat stress and chronic dehydration, exacerbated by the changing climate. Farmers in the North Central and Eastern provinces work long hours under an unforgiving sun, often without access to adequate quantities of clean drinking water.
There is growing evidence that repeated episodes of acute kidney injury caused by dehydration can lead to the permanent interstitial fibrosis characteristic of CKDu. This theory connects the Sri Lankan experience with similar ‘Mesoamerican Nephropathy’ seen among sugarcane workers in Central America, suggesting that CKDu may be a global phenomenon tied to the physical realities of manual labour in warming tropical climates. As global temperatures rise, the ‘heat stress’ hypothesis gains more urgency, positioning the Sri Lankan crisis not just as a local medical mystery, but as an early warning sign of how climate change impacts the health of the global agrarian workforce.
Geographical expansion of disease
The geographic expansion of the disease is a significant concern for the Ministry of Health in 2026. While Anuradhapura remains the epicentre, new ‘hotspots’ have been identified in the Uva and Northwestern provinces, as well as parts of the Southern hinterlands. This spread suggests that the environmental or behavioural triggers are more widespread than previously thought or that the migration of labour and changing agricultural practices are carrying the risk factors into new territories. The government has responded by shifting its strategy toward a more decentralized model of care. The establishment of the Specialized Nephrology Hospital in Polonnaruwa was a landmark achievement, providing state-of-the-art facilities for transplantation and dialysis. However, the sheer volume of patients means that the burden on tertiary care centres remains unsustainable. Consequently, the focus has shifted toward early detection through mobile screening units and the empowerment of primary healthcare centres to manage the early stages of the disease through aggressive blood pressure control and dietary management.
Water Security
Water security has become the primary defensive strategy in the national fight against CKDu. The widespread installation of Reverse Osmosis (RO) plants across high-risk villages has been a transformative community-led intervention. These plants provide filtered water that is significantly lower in mineral content and potential toxins compared to traditional shallow wells. While the long-term efficacy of RO water in preventing new cases is still being evaluated through longitudinal studies, there is strong anecdotal and preliminary evidence suggesting a decline in the rate of new diagnoses in villages that have had consistent access to filtered water for over a decade.
However, the maintenance of these plants remains a challenge, as rural communities often lack the technical expertise or the consistent funding required to replace membranes and ensure the water remains safe for consumption over the long term.
Beyond the biological and environmental dimensions, the CKD situation in Sri Lanka is deeply tied to the social fabric and the psychological well-being of the rural population. There is a profound stigma attached to the disease; in some areas, families hide a diagnosis for fear that it will affect the marriage prospects of their children or lead to social isolation.
This fear often drives patients toward traditional healers or unregulated ‘cures,’ which can sometimes exacerbate kidney damage through the use of heavy-metal-rich herbal preparations. Addressing the ‘fear factor’ through community education and the normalization of regular screening is as essential as any medical treatment. Furthermore, the mental health of caregivers—often women who must balance farming, household duties, and the intensive care of a bedridden relative—is a neglected aspect of the crisis that requires urgent policy attention.
Need for paradigm shift
As we look toward the future, the resolution of the CKD crisis in Sri Lanka will require a paradigm shift in how the state manages its agricultural and environmental resources. The transition toward organic or ‘low input’ farming is being discussed not just as an ecological goal, but as a public health necessity to reduce the chemical load on the soil and water. Simultaneously, the push for universal access to pipe-borne water is the only permanent solution to the groundwater problem. The current situation in 2026 is one of cautious optimism tempered by the reality of a massive existing patient load. While the ‘mystery’ of CKDu may never be reduced to a single cause, the integrated approach of clean water, early detection, and social support offers a roadmap for mitigating the impact of this devastating epidemic.
The resilience of the Sri Lankan farming communities, supported by robust scientific research and empathetic governance, remains the greatest asset in overcoming a disease that has for too long defined the landscape of the Dry Zone.
The Northwestern Province of Sri Lanka, particularly within the districts of Kurunegala and Puttalam, has emerged as a critical front in the national battle against chronic kidney disease. Unlike the early epicentre in the North Central Province, the Northwestern region faced a delayed but rapid surge in cases, largely attributed to its unique hydro-geochemical profile.
The groundwater in areas such as Polpithigama and Nikaweratiya is characterized by high levels of calcium and magnesium, leading to extreme water hardness that, when coupled with fluoride, has been statistically linked to accelerated renal damage. As of 2026, the strategy for this province has shifted from reactive medical treatment to a massive expansion of safe drinking water infrastructure, reflecting a policy acknowledgment that the quality of the ‘input’ into the human body is the single most controllable variable in the CKD epidemic.
Clean water projects
Central to this effort is the National Water Supply and Drainage Board’s Regional Support Centre for the North-Western Province, which has accelerated its goal of achieving near-universal pipe-borne water coverage. A primary focus has been the Anamaduwa Integrated Water Supply Project, a multi-billion-rupee initiative designed to serve over 80,000 residents across the most vulnerable divisions. By transitioning communities away from shallow, untreated agricultural wells and toward centralized, treated surface water systems, the project aims to bypass the nephrotoxic minerals inherent in the local bedrock. This shift is not merely a matter of convenience; it is a life-saving intervention. Early longitudinal data from 2024 and 2025 suggests that in villages where pipe-borne water has replaced groundwater as the primary source for over five years, the rate of new Stage 1 CKDu diagnoses has begun to plateau, providing the first tangible evidence that infrastructure development can decouple agricultural livelihoods from the risk of kidney failure.
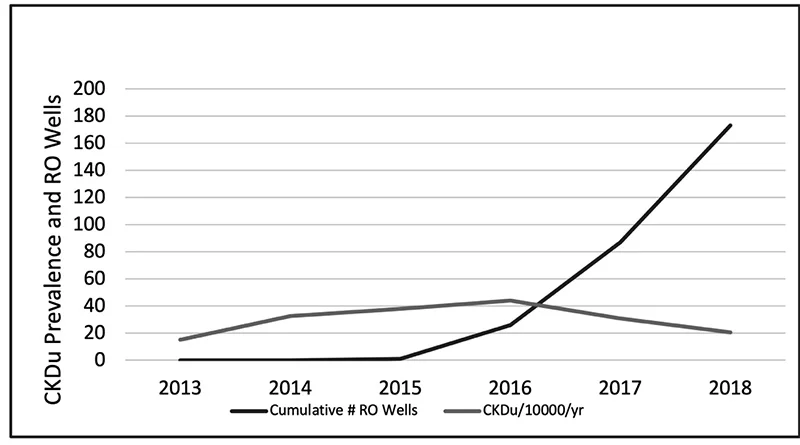
Reverse Osmosis Water Supply Wells and The Reduction of Incidence of CKDu in the North central Province (Source: Kidney disease, health, and commodification of drinking water: An anthropological inquiry into the introduction of reverse osmosis water in the North Central Province of Sri Lanka by de Silva and Albert 2021)
Indispensability of RO plants
While large-scale projects provide a long-term solution, the ‘interim’ role of community-based Reverse Osmosis (RO) plants remains indispensable in the Northwestern hinterlands. These plants, often managed by local community-based organizations (CBOs) with technical oversight from the government, serve as the primary defence for remote settlements that the pipe-borne network has yet to reach. The operational success of these RO plants is increasingly tied to a new model of ‘Water Safety Trust.’
Surveys conducted in 2025 indicate that the reduction of CKD in these areas depends heavily on consistent maintenance; when filters are changed regularly and brine disposal is managed correctly, the resulting ‘soft’ water significantly reduces the metabolic stress on the kidneys of the local farming population. However, the province still faces the challenge of ‘water commodification,’ where the cost of filtered water can occasionally burden the poorest families, highlighting the need for continued state subsidies to ensure that clean water remains a universal right rather than a luxury.
The reduction of CKD in the Northwestern Province is also being driven by a more sophisticated integration of water management and occupational health. Recent initiatives have begun to combine the provision of clean water with ‘cool zones’ and hydration advocacy for farmers working in the intensive heat of the dry zone. There is an increasing understanding that it is not just the quality of water that matters, but the quantity and timing of consumption to prevent the sub-clinical acute kidney injuries that precede chronic failure. By 2026, the regional health authorities have integrated water quality testing with mobile renal screening,
creating a data-driven approach where water projects are prioritized for ‘red-zone’ villages showing the highest incidence of early-stage disease. This holistic strategy marks a transition from viewing CKD as a medical mystery to treating it as a manageable environmental health hazard, with the Northwestern Province serving as a vital testing ground for these integrated interventions.
Biochemical landscape
The biochemical landscape of the Northwestern Province’s water crisis is defined by a sophisticated and lethal interaction between naturally occurring minerals and the human renal system. At the molecular level, the primary concern is the synergistic effect of fluoride ions and water hardness, which is predominantly caused by high concentrations of calcium and magnesium cations. While fluoride is often discussed in isolation, recent research in 2025 and 2026 emphasizes that its toxicity is profoundly amplified when it enters the body through ‘very hard’ water (typically exceeding 180 mg/L of calcium carbonate). When these ions meet in the slightly alkaline environment of the kidney’s proximal tubules, they can form insoluble nanocrystals of calcium fluoride or fluorapatite. These microscopic precipitates act as physical irritants, causing mechanical clogging and chronic inflammation of the delicate tubular basement membranes, eventually leading to the interstitial fibrosis that characterizes CKDu.
Furthermore, the ‘Northwestern profile’ of groundwater often includes the presence of glyphosate—a common herbicide—which scientists now believe acts as a carrier or ‘chelating agent.’ Glyphosate has the chemical ability to bind with calcium and magnesium ions in hard water, forming stable complexes that may protect the toxic elements from being filtered out by the body’s natural defences, allowing them to reach the kidneys in higher concentrations. This ‘Trojan Horse’ mechanism suggests that the disease is not caused by a single pollutant, but by a geochemical cocktail where the hardness of the water essentially ‘primes’ the body to be more susceptible to other environmental toxins. Interestingly, some studies have noted that magnesium-rich water may actually offer a slight protective effect compared to calcium-dominant water, suggesting that the specific ratio of minerals in a village’s well could determine its status as a ‘hotspot’ or a safe zone.
To combat these complex interactions, the maintenance of Reverse Osmosis (RO) plants has become a cornerstone of rural health policy, though it remains fraught with logistical challenges. As of 2026, the Ministry of Health has moved toward a ‘Uniform Regulation and Training’ model to address the high variability in water quality produced by community-managed plants. Without precise maintenance, RO membranes can become ‘fouled’ by the very minerals they are designed to remove, leading to a precipitous drop in filtration efficiency. Policy experts now advocate for a ‘Public-Private-Community Partnership’ where the government provides the technical sensors and remote monitoring technology, while local organizations handle day-to-day operations. This ensures that the Total Dissolved Solids (TDS) levels remain consistently below the 30-ppm threshold required to effectively ‘reset’ the mineral balance for residents who have spent decades consuming the region’s hazardous groundwater.
Fruitful environmental intervention
Ultimately, the reduction of CKD in the Northwestern Province is a testament to the power of targeted environmental intervention. By treating the water supply as a biological variable rather than just a utility, Sri Lanka is creating a global blueprint for managing ‘geogenic’ diseases. The transition from the ‘shallow regolith aquifers’—which are highly susceptible to both natural mineral leaching and agricultural runoff—to deeper, treated surface water sources represents the most significant shift in the province’s public health history. As these infrastructure projects reach completion, the hope is that the next generation of farmers in Kurunegala and Puttalam will be the first in decades to work their land without the looming shadow of a silent, water-borne epidemic.

The US Government has gifted 10 Bell 206, Sea Ranger Helicopters to the SLAF for Training and Humanitarian Assistance and Disaster Relief (HADR) purposes. The full specifications are as follows.
Contractor:
Bell Helicopter Textron
Date Deployed: First flight: 1961; Operational: 1968
Propulsion: One Allison 250-C20BJ turbofan engine
Length: Fuselage – 31 feet (9.44 meters); Rotors turning – 39 feet (11.9 meters)
Height: 10 feet (3.04 meters)
Rotor Diameter: 35 feet 4 inches (10.78 meters)
Weight: 1595 pounds (725kg) empty, 3200 pounds (1455 kg) maximum take-off
Airspeed: 138 miles (222 km) per hour maximum; 117 miles (188 km) per hour cruising
Ceiling: 18,900 feet (5,761 meters)
Range: 368 nautical miles (420 statute miles, 676 km)
Crew: One pilot, four students
While they are good for training, I have my serious doubts whether these helicopters are ideal for HADR. As they have only a single engine and They can’t even operate into high rise helipads in hospitals and hotels in Colombo. The law requires twin engine helicopters! What happens if there is an engine failure while operating over the sea or in a mountainous area? There will be hell to pay!
Three twin engine versions would have been better.
How many helicopter pilots does the SLAF require anyway?
Will we be stuck with junk? Like two Russian KA -26’s during the Sirimavo Government and French Aerospatiale Dauphins SLAF acquired. which were not ‘tropicalised’, during the JRJ Government.
Will the Sea Ranger Spares support be available, free of charge?
I doubt it.
There will also be other Geopolitical strings attached. There is no such thing as a free lunch.
Guwan Seeya

Global warming policies were expected to drive a rapid shift toward a renewables-based energy system dominated by wind and solar. While growth in these sources did occur, it has not matched the pace that was widely anticipated. In the United States, the rise of cheap and abundant shale natural gas significantly reshaped the energy mix, displacing coal and limiting the relative share of wind and solar in electricity generation. In China and India, the situation has been different.
Coal remains dominant because it is widely available domestically, while natural gas is more limited or expensive to secure at scale. As a result, coal has retained its central role in both countries’ power systems. Solar and wind always provide intermittent, variable power. It was widely assumed that a cost-effective, utility-scale electricity storage solution would emerge to solve this problem, but that has not yet happened at the scale originally expected. In the pre-AI era, solar and wind were typically integrated into power systems alongside more reliable sources such as coal, natural gas, and nuclear energy.
For example, if the sun was shining on a Monday, electricity demand could be met largely by solar power during the day. At night, coal, natural gas, or nuclear plants would supply the required electricity. If the following Tuesday was cloudy or gloomy, generation would shift back toward coal, gas, or nuclear to maintain supply. AI introduces a new and more demanding challenge. AI data centers require continuous, high-quality, always-on electricity, which solar and wind alone struggle to guarantee without large-scale storage or back-up systems. In addition, they require very large amounts of power.
As a result, the AI industry is now actively searching for new and expanded sources of reliable electricity. One of the major challenges in powering AI systems is electricity transmission. High-voltage transmission lines are expensive, slow to build, and often face regulatory and land-use constraints. As a result, some companies are exploring more localized power solutions, sometimes referred to as microgrids. These are self-contained energy systems that can operate independently from the main electricity grid. Technologies such as small modular nuclear reactors are an example of such microgrids.
In such isolated systems, the focus is on highly reliable, always available power generated close to the point of use. In this context, solar and wind are expected to play a limited role because their output is variable and depends on weather conditions, making them less suited as primary sources in fully self-contained AI-focused microgrids. The pace of AI infrastructure development is extremely rapid in both the United States and China. AI systems are widely seen as transformative technologies that promise significant new wealth creation, which is driving aggressive and sustained investment. As a result, development is moving quickly, without waiting for long-term solutions such as large-scale energy storage to mature alongside renewable energy systems.
In this environment, electricity demand is rising faster than new infrastructure can be built. In the United States, this reinforces the role of natural gas as the dominant source of reliable power. In China and India, where coal remains more established and readily available, it is likely to continue playing a central role in meeting growing demand. In India, AI data centers have not yet been built at the scale seen in the United States and China. When India does reach that stage, it will need to supply large amounts of reliable electricity. India has placed strong emphasis on solar energy in particular and has had some success in meeting the needs of ordinary consumers through renewable expansion. However, the key question is what choices will be made when large-scale AI data centers begin to arrive.
Will India rely more on coal generation, which is relatively cheap, widely available, and highly reliable, or on solar power, which is intermittent, variable, and often more expensive when reliability is taken into account? My view is that India is more likely to turn to coal to meet this demand, given its existing infrastructure and the need for dependable electricity supply. Then there is an overall question. Solar and wind were already struggling in the pre-AI days to displace coal and natural gas at the system level, despite strong expectations that they would become dominant sources of electricity. Now that AI is here and electricity demand is rising rapidly, will they push solar and wind further behind in the energy mix? (The Statesman)
(The writer is an expert on energy and contributes regularly to publications in India and overseas.)
by SUNIL SHARAN

Celebrating the Life and Legacy of Dr Naomal P. S. Gunaratna 10 January 1931 – 07 May 2026
When a colossus of human virtue departs this earthly theatre, the silence left in its wake is not merely the absence of sound, but a profound, resonant reverberation that echoes through the very corridors of our souls. On that most distressing 07 of May, 2026, the mortal final curtain fell upon the magnificent, multi-faceted tapestry of a life lived to its exquisite pinnacle. Dr Naomal P. S. Gunaratna, having completed a glorious earthly sojourn of ninety-five years, surrendered his gentle spirit to the infinite, leaving behind a world demonstrably poorer for his departure.
To speak of him is to speak of an absolute gem of humanity, a mortal who walked among us with the quiet majesty of a king, the tender heart of a saint, and the flawless grace of a true nobleman. He was a Consultant Paediatrician of peerless distinction. Yet for all that, well above and beyond the glittering accolades of his noble vocation, he was, in the truest and most sublime sense of the phrase, a human being par excellence.
In attempting to encapsulate the vast depth of Naomal’s character, even the richness of the English language feels frustratingly inadequate, compelling one to search for words forged in the fires of profoundest reverence. He was a grandee possessed of sterling qualities so rare in this modern transactional era that his presence felt like an exquisite anachronism; a beautiful remainder of an age when honour was a man’s sanctuary, and integrity was his unwavering Northern Star. His uniqueness did not stem from an assertive, ostentatious display of superiority. It blossomed from the quiet, luminous radiance of an authentic soul. To have been counted among his close friends is a privilege of such monumental proportions that it stands as one of the most radiant blessings of my own life. Our bond was not woven from the fragile threads of casual acquaintance, but forged in the durable crucible of mutual respect, shared ideals, and a deep, unspoken understanding of the beauty inherent in lives dedicated to the service of others.
In an age where the ethical landscape is all too often obscured by the shifting mists of compromise and moral ambivalence, Naomal stood like an unyielding granite cliff against the turbulent seas of opportunism. His rectitude was absolute, non-negotiable, and entirely independent of an audience. He did what was right, not for the fleeting warmth of public adulation, but because his internal moral compass was tuned to an otherworldly frequency. His word was a sacred covenant, an unbreakable bond that required no legal seal or written witness. In his professional life as a Consultant Paediatrician, this supreme integrity manifested as an unswerving commitment to the highest principles of Hippocratic devotion. He was a healer who could neither be bought nor swayed by the seductive allure of material gain or institutional politics. He wielded his stethoscope not as an instrument of commerce, but as a sacred conduit of compassion, bridging the divide between clinical expertise and the tender vulnerabilities of human suffering.
How can one adequately depict the soft, enveloping warmth of a heart that beats in perpetual symphony with the distress of others? Naomal’s benevolence was not a performative gesture, nor was it a duty executed with cold, clinical precision. It was an effusive, spontaneous overflow of pure, unadulterated love. It was a kindness that possessed its own unique atmosphere, a soothing gentleness that disarmed fear and banished despair. When he entered a room, the emotional temperature invariably rose, thawed by the genuine, sparkling warmth of his magnificent smile. His eyes, windows to a soul completely devoid of malice, mirrored a profound empathy that could diagnose a broken spirit as swiftly as a physical ailment.
He was brought up in his early days at De Mazenod College in Kandana, St Peter’s College Colombo, Royal College Colombo, and during the period of World War II, in Glendale College, Bandarawela. In a glittering career that followed specialisation in paediatrics, he has worked in the Government Hospital in Gampaha and Kuliyapitiya, the Department of Paediatrics of the University of Peradeniya, North Colombo Medical College in Ragama and then at the Department of Paediatrics of the University of Kelaniya. To the thousands of children who passed through his healing hands across the decades, he was not merely a doctor in a sterile white coat; he was a grand, benevolent guardian angel, a comforting presence whose very touch possessed an alchemy that turned terror into tranquillity and tears into triumphant laughter. To scores of his students, he was a father figure, a mentor and a brilliant teacher. In the years gone by, he was the President of the Sri Lanka Paediatric Association, which is now the Sri Lanka College of Paediatricians, President of the Vaccines and Infectious Diseases Forum of Sri Lanka and a much-valued Council Member of the Independent Medical Practitioners Association (IMPA). The unblemished finesse that he exhibited in these positions is indeed an abiding lesson to all and sundry.
As a Consultant Paediatrician, Naomal’s brilliance was legendary, a beacon of excellence that illuminated the medical fraternity. Yet, his profound intellect was beautifully balanced by an equal measure of humility. He possessed the rare ability to untangle the most knotty, complex medical conundrums with a swift, intuitive diagnostic precision, all while maintaining a bedside manner that was as gentle as a summer breeze. He understood, with a depth that bypassed mere textbook knowledge, that a sick child is a fragile ecosystem, intertwined with the agonising anxieties of distraught parents. Consequently, his consultations were masterclasses in holistic healing. He did not merely treat a disease; he cradled a family. He would spend hours patiently explaining clinical intricacies to frightened mothers, his voice a calm, reassuring anchor in the midst of their emotional storms. He treated the children of royalty and the children of peasants, with the same meticulous care, the same overflowing affection, and the same absolute dedication, recognising the identical, priceless spark of divinity within each innocent soul.
A personal anecdote goes to show the most admirable and true spirit of the man. I did not know Naomal from Adam till 1990. In January of 1990, following my tenure of office in General Hospital Badulla, General Hospital Ratnapura and General Hospital Kurunegala, I was posted as the Consultant Paediatrician to Kalubowila Hospital by the Ministry of Health. Both Naomal and I did our Private Consultations at Asiri Medical Hospital. We worked on the same floor and became really close friends. He had loads of patients, while I had extremely few, as I was totally unknown. Most of the time, I was seated in my Consulting Room, twiddling my thumbs and waiting for some tangible work with children.
Then one day, Naomal came to my room and said that he needed to go abroad for an extended period of about six to eight months and asked me whether I could look after his patients. I was very happy to do it as at that time, as it was like ‘manna from heaven’ for me. So, it went on, I looked after his little patients, and I was financially the richer for it.
Then, when Naomal came back after all those months, I told all his patients that I was only covering up his work and that they should go back to him. However, some of them wanted to stay with me. I told them that the only way in which I would continue to look after their children was for them to get a note to that effect from Dr Naomal Gunaratna. I was quite sure that it would not come to pass that way. They went to him and told him what I said, and Naomal, most nonchalantly, graciously and with the greatest pleasure, issued a little note to each of them in which he had written “My dear BJC, please be kind enough to take over the care of this child“. Need I say more? What a man? What a fantastic person who showed by his quiet deeds that his values transcended petty considerations and monetary reflections?
The longevity of ninety-five years is a milestone granted only to a few. For Naomal, these nine decades plus were not merely a passive accumulation of days but a grand, purposeful march through time. He aged with an unparalleled, majestic dignity, his wisdom deepening like a fine vintage, while his youthful enthusiasm for life remained entirely unextinguished by the passing years. Even as his physical frame grew frail under the inevitable weight of time, his mind remained a brilliant, caerulean laboratory of thought, and his spirit retained its effervescent, childlike joy. He never allowed the cynicism of an evolving world to pollute the pristine waters of his optimism. To sit with him in his twilight years was to drink from a fountain of pure, unvarnished wisdom. He looked back upon his long journey not with the wistful regrets of a man mourning, but with the serene, tranquil satisfaction of an accomplished master craftsman who looks upon a masterpiece and knows he has given it his all, in the finest sense of the phrase.
We must also celebrate the quiet, understated grandeur of his private universe. Naomal was a man of exquisite tastes, an intellectual who found solace in the harmony of great literature, the majesty of classical arts, and the quiet contemplation of nature’s wonders. Yet, his greatest joy was found in the warmth of human connections. He was a loyal, fiercely protective friend, a steadfast pillar of strength upon whom one could lean with absolute confidence, even during life’s most turbulent seasons. In an era dominated by superficial relationships and digital illusions, his friendship was a solid, tangible sanctuary. His conversations were never trivial; they were rich and multi-layered tapestries woven with historical anecdotes, medical philosophies, gentle humour, and profound spiritual insights. To converse with him was to be elevated, and to be challenged to think more deeply, love more expansively, and live more honourably.
On that day of his departure from this mortal world, the world lost an exceptional treasure. The medical profession lost one of its most venerable elder statesmen, humanity lost an exemplary ambassador, and I lost a cherished brother of the heart. The grief we feel is heavy, a dark and suffocating shroud that threatens to overwhelm us. Yet, as we stand in the shadow of this monumental loss, we must not weep as those who have no hope. Naomal’s demise is not an absolute end but a glorious transition. It is the triumphant homecoming of a soul that has magnificently fulfilled its earthly mandate. The physical vessel which carried his inner being may return to the dust from which it came, but the essence of who he was, the kindness he disseminated, the lives he saved, the love he kindled, and the pristine integrity he modelled remain forever immortalised in the fabric of our realities.
He has crossed the ultimate horizon, entering that everlasting realm where pain is obsolete, and peace reigns eternal. We can almost see him now, walking through fields of everlasting light, his countenance radiant, his step light and free, greeted by a chorus of godly beings and even the grateful souls of the children he mended but who preceded him into eternity. The man has fought the good fight, he has finished the race, he has kept the faith with absolute, unyielding fidelity. His life was a beautiful, symphonic ensemble dedicated to the upliftment of humans, and its final stanza, though hushed in death, is an abiding opus which leaves an eternal melody playing in our hearts.
Farewell, my dearly beloved friend; goodbye, Dr Naomal P. S. Gunaratna. You were an absolute gem of a person, a human being par excellence, and a star that burned with a brilliant, comforting light in our earthly sky. Though you have gone away from our sight, your luminescence will continue to guide our steps through the gathering shadows until that glorious dawn when we shall meet again on the farther shore.
May your most beautiful, noble soul rest in eternal, serene, and uninterrupted peace. May you attain eternal bliss!
I conclude with the immortal words, as depicted by the great bard William Shakespeare in Julius Caesar (Act V, Scene 5) “His life was gentle, and the elements so mixed in him that nature might stand up and say to all the world, This was a man.”
By Dr B. J. C. Perera
Specialist Consultant Paediatrician


Diesel replacement costs up to Rs. 4.5 bn in April

Sallay on hunger strike: Counsel warns CID

Opp. questions why Rs 10 bn meant for Ditwah victims held in Treasury account

‘Samurdhi Bank operates without dedicated audit framework’

Constitutional inconsistencies relating to franchise

‘Dates have the highest sugar content to fight Coronavirus’

Sunday Island 27 December – Headlines

#SundayIsland 17th December – Headlines

Sunday Island – 28th March

Sunday Island Headlines – 21 March

Sunday Island – 21st February – Headlines
-

 News6 days ago
News6 days agoLankan duo emerge winners in Latin dance championship held in Blackpool, UK
-

 Latest News4 days ago
Latest News4 days agoKusal Mendis, Pathum Nissanka, bowlers put Sri Lanka 1-0 up
-

 News4 days ago
News4 days agoNew US tariffs proposed on 60 countries, including Sri Lanka
-

 Features3 days ago
Features3 days agoPower crept into the Sangha and is now tearing it apart
-

 News6 days ago
News6 days agoSri Lankan teen killed in Chennai clash; three arrested
-

 Features3 days ago
Features3 days agoKondachchi wind farm and battery storage project to boost energy security, says Power Ministry Secretary
-

 Features3 days ago
Features3 days agoSaudi Arabia sets new benchmark in Hajj management as 1.7 million pilgrims complete sacred journey
-

 News2 days ago
News2 days agoAsst. Manager, security officer arrested over Rs 30 mn snatch at Horana PB branch