Opinion
Social and Biological Landscape of Kidney Disease in Sri Lanka
World Kidney Day falls today
The Chronic Kidney Disease (CKD) crisis in Sri Lanka represents one of the most formidable public health challenges of the twenty-first century, manifesting as a complex tapestry of environmental, social, and physiological factors. Unlike the traditional forms of kidney disease seen in urban centres—which typically stem from well-understood comorbidities like long-term diabetes and hypertension—the situation in the Sri Lankan ‘Dry Zone’ is defined by a mysterious and aggressive variant known as Chronic Kidney Disease of unknown aetiology (CKDu). This specific form of the disease has devastated the agricultural heartlands, particularly the North Central Province, for over three decades, yet it continues to evolve in its geographic reach and its socio-economic impact as of 2026. The persistence of this epidemic despite extensive international research highlights a profound gap in our understanding of how tropical environments and traditional occupational hazards intersect to damage human renal systems.
Historically, the emergence of CKDu was first noted in the late 1990s around the Anuradhapura and Polonnaruwa districts. What began as sporadic cases in rural hospitals quickly transformed into a localized epidemic, catching the medical community off guard because the patients did not present with the usual risk factors. These were not the sedentary, elderly populations usually associated with renal failure; rather, they were lean, active, middle-aged rice farmers.
The demographic specificity of the disease remains a chilling hallmark of the crisis today. It predominantly strikes men during their peak productive years, which triggers a catastrophic ripple effect through the family unit. When a primary breadwinner in a subsistence farming household falls ill, the family is thrust into a ‘poverty trap’ where limited resources are redirected toward transport to distant clinics, expensive nutritional supplements, and eventually, the gruelling routine of dialysis. This economic erosion often forces children out of school and into labour, perpetuating a cycle of systemic vulnerability that lasts for generations.
Intense scientific debate
The aetiology of the disease remains a subject of intense scientific debate and is currently viewed through a multifactorial lens. Researchers have moved away from the search for a single ‘smoking gun’ and are instead examining a lethal synergy of environmental triggers. Groundwater quality remains at the forefront of this investigation. The dry zone of Sri Lanka is characterized by high levels of fluoride and groundwater hardness, and it is theorized that the interaction between these natural minerals and anthropogenic pollutants—such as heavy metals from agrochemicals—creates a nephrotoxic cocktail.
The historical reliance on chemical fertilizers and pesticides in the ‘Green Revolution’ era of Sri Lankan agriculture is often cited as a major contributing factor. While direct links to specific brands of pesticides have been difficult to prove definitively, the accumulation of cadmium, arsenic, and lead in the soil and food chain continues to be monitored as a primary catalyst for the slow, progressive scarring of the kidney tubules.
In recent years, the discourse around CKDu has expanded to include the role of heat stress and chronic dehydration, exacerbated by the changing climate. Farmers in the North Central and Eastern provinces work long hours under an unforgiving sun, often without access to adequate quantities of clean drinking water.
There is growing evidence that repeated episodes of acute kidney injury caused by dehydration can lead to the permanent interstitial fibrosis characteristic of CKDu. This theory connects the Sri Lankan experience with similar ‘Mesoamerican Nephropathy’ seen among sugarcane workers in Central America, suggesting that CKDu may be a global phenomenon tied to the physical realities of manual labour in warming tropical climates. As global temperatures rise, the ‘heat stress’ hypothesis gains more urgency, positioning the Sri Lankan crisis not just as a local medical mystery, but as an early warning sign of how climate change impacts the health of the global agrarian workforce.
Geographical expansion of disease
The geographic expansion of the disease is a significant concern for the Ministry of Health in 2026. While Anuradhapura remains the epicentre, new ‘hotspots’ have been identified in the Uva and Northwestern provinces, as well as parts of the Southern hinterlands. This spread suggests that the environmental or behavioural triggers are more widespread than previously thought or that the migration of labour and changing agricultural practices are carrying the risk factors into new territories. The government has responded by shifting its strategy toward a more decentralized model of care. The establishment of the Specialized Nephrology Hospital in Polonnaruwa was a landmark achievement, providing state-of-the-art facilities for transplantation and dialysis. However, the sheer volume of patients means that the burden on tertiary care centres remains unsustainable. Consequently, the focus has shifted toward early detection through mobile screening units and the empowerment of primary healthcare centres to manage the early stages of the disease through aggressive blood pressure control and dietary management.
Water Security
Water security has become the primary defensive strategy in the national fight against CKDu. The widespread installation of Reverse Osmosis (RO) plants across high-risk villages has been a transformative community-led intervention. These plants provide filtered water that is significantly lower in mineral content and potential toxins compared to traditional shallow wells. While the long-term efficacy of RO water in preventing new cases is still being evaluated through longitudinal studies, there is strong anecdotal and preliminary evidence suggesting a decline in the rate of new diagnoses in villages that have had consistent access to filtered water for over a decade.
However, the maintenance of these plants remains a challenge, as rural communities often lack the technical expertise or the consistent funding required to replace membranes and ensure the water remains safe for consumption over the long term.
Beyond the biological and environmental dimensions, the CKD situation in Sri Lanka is deeply tied to the social fabric and the psychological well-being of the rural population. There is a profound stigma attached to the disease; in some areas, families hide a diagnosis for fear that it will affect the marriage prospects of their children or lead to social isolation.
This fear often drives patients toward traditional healers or unregulated ‘cures,’ which can sometimes exacerbate kidney damage through the use of heavy-metal-rich herbal preparations. Addressing the ‘fear factor’ through community education and the normalization of regular screening is as essential as any medical treatment. Furthermore, the mental health of caregivers—often women who must balance farming, household duties, and the intensive care of a bedridden relative—is a neglected aspect of the crisis that requires urgent policy attention.
Need for paradigm shift
As we look toward the future, the resolution of the CKD crisis in Sri Lanka will require a paradigm shift in how the state manages its agricultural and environmental resources. The transition toward organic or ‘low input’ farming is being discussed not just as an ecological goal, but as a public health necessity to reduce the chemical load on the soil and water. Simultaneously, the push for universal access to pipe-borne water is the only permanent solution to the groundwater problem. The current situation in 2026 is one of cautious optimism tempered by the reality of a massive existing patient load. While the ‘mystery’ of CKDu may never be reduced to a single cause, the integrated approach of clean water, early detection, and social support offers a roadmap for mitigating the impact of this devastating epidemic.
The resilience of the Sri Lankan farming communities, supported by robust scientific research and empathetic governance, remains the greatest asset in overcoming a disease that has for too long defined the landscape of the Dry Zone.
The Northwestern Province of Sri Lanka, particularly within the districts of Kurunegala and Puttalam, has emerged as a critical front in the national battle against chronic kidney disease. Unlike the early epicentre in the North Central Province, the Northwestern region faced a delayed but rapid surge in cases, largely attributed to its unique hydro-geochemical profile.
The groundwater in areas such as Polpithigama and Nikaweratiya is characterized by high levels of calcium and magnesium, leading to extreme water hardness that, when coupled with fluoride, has been statistically linked to accelerated renal damage. As of 2026, the strategy for this province has shifted from reactive medical treatment to a massive expansion of safe drinking water infrastructure, reflecting a policy acknowledgment that the quality of the ‘input’ into the human body is the single most controllable variable in the CKD epidemic.
Clean water projects
Central to this effort is the National Water Supply and Drainage Board’s Regional Support Centre for the North-Western Province, which has accelerated its goal of achieving near-universal pipe-borne water coverage. A primary focus has been the Anamaduwa Integrated Water Supply Project, a multi-billion-rupee initiative designed to serve over 80,000 residents across the most vulnerable divisions. By transitioning communities away from shallow, untreated agricultural wells and toward centralized, treated surface water systems, the project aims to bypass the nephrotoxic minerals inherent in the local bedrock. This shift is not merely a matter of convenience; it is a life-saving intervention. Early longitudinal data from 2024 and 2025 suggests that in villages where pipe-borne water has replaced groundwater as the primary source for over five years, the rate of new Stage 1 CKDu diagnoses has begun to plateau, providing the first tangible evidence that infrastructure development can decouple agricultural livelihoods from the risk of kidney failure.
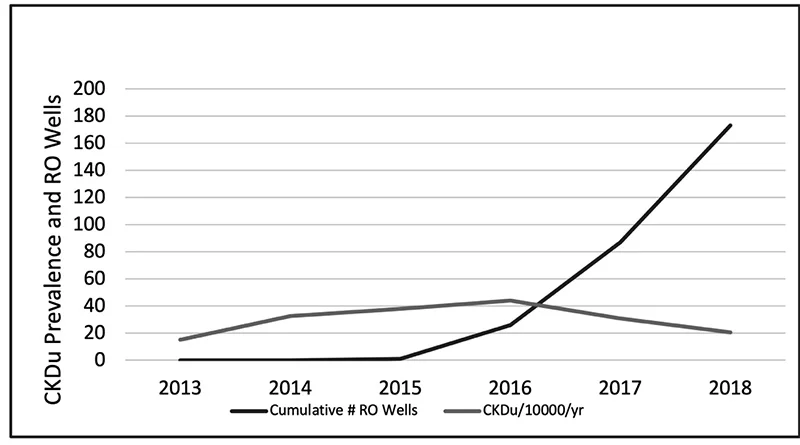
Reverse Osmosis Water Supply Wells and The Reduction of Incidence of CKDu in the North central Province (Source: Kidney disease, health, and commodification of drinking water: An anthropological inquiry into the introduction of reverse osmosis water in the North Central Province of Sri Lanka by de Silva and Albert 2021)
Indispensability of RO plants
While large-scale projects provide a long-term solution, the ‘interim’ role of community-based Reverse Osmosis (RO) plants remains indispensable in the Northwestern hinterlands. These plants, often managed by local community-based organizations (CBOs) with technical oversight from the government, serve as the primary defence for remote settlements that the pipe-borne network has yet to reach. The operational success of these RO plants is increasingly tied to a new model of ‘Water Safety Trust.’
Surveys conducted in 2025 indicate that the reduction of CKD in these areas depends heavily on consistent maintenance; when filters are changed regularly and brine disposal is managed correctly, the resulting ‘soft’ water significantly reduces the metabolic stress on the kidneys of the local farming population. However, the province still faces the challenge of ‘water commodification,’ where the cost of filtered water can occasionally burden the poorest families, highlighting the need for continued state subsidies to ensure that clean water remains a universal right rather than a luxury.
The reduction of CKD in the Northwestern Province is also being driven by a more sophisticated integration of water management and occupational health. Recent initiatives have begun to combine the provision of clean water with ‘cool zones’ and hydration advocacy for farmers working in the intensive heat of the dry zone. There is an increasing understanding that it is not just the quality of water that matters, but the quantity and timing of consumption to prevent the sub-clinical acute kidney injuries that precede chronic failure. By 2026, the regional health authorities have integrated water quality testing with mobile renal screening,
creating a data-driven approach where water projects are prioritized for ‘red-zone’ villages showing the highest incidence of early-stage disease. This holistic strategy marks a transition from viewing CKD as a medical mystery to treating it as a manageable environmental health hazard, with the Northwestern Province serving as a vital testing ground for these integrated interventions.
Biochemical landscape
The biochemical landscape of the Northwestern Province’s water crisis is defined by a sophisticated and lethal interaction between naturally occurring minerals and the human renal system. At the molecular level, the primary concern is the synergistic effect of fluoride ions and water hardness, which is predominantly caused by high concentrations of calcium and magnesium cations. While fluoride is often discussed in isolation, recent research in 2025 and 2026 emphasizes that its toxicity is profoundly amplified when it enters the body through ‘very hard’ water (typically exceeding 180 mg/L of calcium carbonate). When these ions meet in the slightly alkaline environment of the kidney’s proximal tubules, they can form insoluble nanocrystals of calcium fluoride or fluorapatite. These microscopic precipitates act as physical irritants, causing mechanical clogging and chronic inflammation of the delicate tubular basement membranes, eventually leading to the interstitial fibrosis that characterizes CKDu.
Furthermore, the ‘Northwestern profile’ of groundwater often includes the presence of glyphosate—a common herbicide—which scientists now believe acts as a carrier or ‘chelating agent.’ Glyphosate has the chemical ability to bind with calcium and magnesium ions in hard water, forming stable complexes that may protect the toxic elements from being filtered out by the body’s natural defences, allowing them to reach the kidneys in higher concentrations. This ‘Trojan Horse’ mechanism suggests that the disease is not caused by a single pollutant, but by a geochemical cocktail where the hardness of the water essentially ‘primes’ the body to be more susceptible to other environmental toxins. Interestingly, some studies have noted that magnesium-rich water may actually offer a slight protective effect compared to calcium-dominant water, suggesting that the specific ratio of minerals in a village’s well could determine its status as a ‘hotspot’ or a safe zone.
To combat these complex interactions, the maintenance of Reverse Osmosis (RO) plants has become a cornerstone of rural health policy, though it remains fraught with logistical challenges. As of 2026, the Ministry of Health has moved toward a ‘Uniform Regulation and Training’ model to address the high variability in water quality produced by community-managed plants. Without precise maintenance, RO membranes can become ‘fouled’ by the very minerals they are designed to remove, leading to a precipitous drop in filtration efficiency. Policy experts now advocate for a ‘Public-Private-Community Partnership’ where the government provides the technical sensors and remote monitoring technology, while local organizations handle day-to-day operations. This ensures that the Total Dissolved Solids (TDS) levels remain consistently below the 30-ppm threshold required to effectively ‘reset’ the mineral balance for residents who have spent decades consuming the region’s hazardous groundwater.
Fruitful environmental intervention
Ultimately, the reduction of CKD in the Northwestern Province is a testament to the power of targeted environmental intervention. By treating the water supply as a biological variable rather than just a utility, Sri Lanka is creating a global blueprint for managing ‘geogenic’ diseases. The transition from the ‘shallow regolith aquifers’—which are highly susceptible to both natural mineral leaching and agricultural runoff—to deeper, treated surface water sources represents the most significant shift in the province’s public health history. As these infrastructure projects reach completion, the hope is that the next generation of farmers in Kurunegala and Puttalam will be the first in decades to work their land without the looming shadow of a silent, water-borne epidemic.
I was taken aback by the response of the well-known academic Uswatte-Aratchi (U-A) to my article “Achievements of the Hunduwa”, which appeared in The Island on 15 March. In his piece, titled “Pot calling the kettle black?” (The Island, 23 April) U-A accuses me of belittling Sri Lanka in just the same way President Anura Kumara Dissanayake (AKD) did with his reference to Sri Lanka as a hunduwa. Being an academic of repute, U-A’s comments cannot be ignored and before I proceed further to explain, let me state that I am very sorry if what I stated appeared in any way to be derogatory; my intentions were otherwise.
U-A states, “Most sensible people, even uneducated, judge that the volume of a little drop (of whatever) is smaller than that of a hunduwa; so is weight. When the learned doctor emphatically maintains ‘we are not a hunduwa’ but ‘a little drop in the ocean’, is the pot calling the kettle black or worse?” He implies that my ‘insult’ is worse. Whilst conceding that a drop is smaller than a hunduwa, what baffles me is how an academic overlooked the fact that comparisons should be made based on context. Whereas AKD used hunduwa in the parliament to belittle the country, I used the term ‘little drop’ to highlight our achievements, which are disproportionate to our size. In contrast, AKD used hunduwa to trifle with the country.
“Surely, this little drop in the Indian ocean performed well beyond its size to have gained international recognition way back in history,” I said in my article. This cannot in any way be considered derogatory. In fact, what U-A stated in his article about the achievements of countries, either smaller or with populations smaller than ours, only supports my view that there is no correlation between a country’s size and its achievements.
U-A casts doubt on the assertion that Sri Lanka was once the ‘Granary of the East’; he cites instances of drought and famine. There may have been bad periods, as we are at the mercy of nature, but it does not negate the fact that there were periods of plenty too. Our rulers in days of yore did everything possible to feed the populace by building tanks and extensive irrigation systems. In addition to major works, there were networks of small projects, Uva being referred to as ‘Wellassa’; the land of one hundred thousand paddy fields fed by small tanks. What has the present government done to ease farmers’ burden? Absolutely nothing! Whilst farmers are struggling to eke out a living, rice millers are importing super-luxury vehicles and even helicopters!
I agree with U-A that unfortunately the contribution of the ordinary people is not well recorded in history. This is a universal problem, not limited to Sri Lanka. When one watches some of Prof. Raj Somadeva’s programmes, it becomes clear how ordinary people helped complete gigantic projects. Although there are many documentaries on how the pyramids were built, no one seems interested in exploring how Great Stupas in Anuradhapura were built with millions of bricks.
AKD is doing just the opposite of what he preached whilst in Opposition and does not seem to have any sense of shame. His hunduwa reference, possibly, makes him the only President to have demeaned the country.
by Dr Upul Wijayawardhana

Recent statements from Washington show how global politics is being increasingly framed along civilisational terms. The U.S. Secretary of State Marco Rubio has referred to the idea of a shared “Western civilisation,” describing the U.S. and Europe as bound by common history, cultural heritage, and institutional traditions. At the same time, U.S. President Donald Trump has amplified comments about countries such as India, China, and Iran in the context of migration and geopolitical competition that reinforce a tendency to interpret global politics in civilisational terms. Taken together, these statements point to a broader shift: global affairs are being interpreted not only through the language of power and interest, but also through civilisational identities.
The appeal of such framing is understandable. It offers a sense of clarity in an era of rapid technological disruption, demographic change, and geopolitical uncertainty. But apparent clarity is not the same as analytical accuracy. Moreover, it is not an entirely new framing either. As early as the 1990s, political scientist Samuel Huntington had argued that global politics would evolve into a “clash of civilisations,” where cultural and religious identities would become the principal fault lines of international relations.
Civilisational explanations can obscure more than they reveal, particularly when they imply that cultural cohesion, rather than institutional adaptability, is the primary source of national strength. A historical record of the modem West suggests otherwise.
A look at history
Much of the West’s post-Cold War dynamism has rested not on homogeneity, but on openness — to talent, ideas, capital, and global competitive pressures. Its advantage has been institutional: the capacity to absorb diversity and convert it into innovation within rules-based systems.
Nowhere is this more evident than in today’s innovation economy. AI, in particular, has become the defining frontier of global competition, shaped by deeply international talent flows and research ecosystems. Companies such as Microsoft, Open Al, and NVIDIA exemplify systems in which breakthroughs depend on globally sourced expertise, cross-border collaboration, and the ability to attract the most capable minds regardless of origin.
The COVID-19 pandemic underscored this complementary reality: innovation now operates through globally distributed production systems. Rapid vaccine development and distribution, by firms such as Modema and AstraZeneca, depended on international research networks and global manufacturing ecosystems. In the case of AstraZeneca, large-scale production through partnerships such as that with the Serum Institute of India illustrated how innovation and industrial capacity now operate across borders.
This is not an argument against immigration control. Immigration must be governed effectively, and civic norms must be upheld. But managing diversity is fundamentally different from retreating from it.
In an era of intensifying geopolitical competition, openness remains a critical strategic asset. The West’s advantage lies not only in military alliances or economic scale, but in institutional resilience and its capacity to attract, integrate, and retain talent. Civilisational framing, by contrast, risks misdiagnosing this advantage —privileging identity over capability and boundaries over performance. Demographic realities reinforce this point. Many advanced economies face ageing populations. In this context, immigration is not simply a cultural or political issue, but an economic necessity.
Without sustained inflows of sldlled labour and human capital, growth slows, fiscal pressures increase, and innovation ecosystems weaken.
Openness as an advantage
The defining challenges of the 21st century —including AI governance and climate change —further highlight the limits of civilisational thinking. These are problems that cannot be addressed within cultural silos. Against this backdrop, framing global politics in terms of civilisational hierarchy carries risks. It encourages a narrowing of identity at precisely the moment when cooperation and adaptability are essential.
The question, therefore, is not whether identity matters. It dearly does. Societies require shared norms, institutional trust, and continuity. The more important question is whether democracies can manage change without losing confidence in the openness that has sustained their development. The strength of the West has historically rested on its ability to combine stability with adaptation — to absorb new influences while preserving core principles such as the rule of law, individual liberty, and accountable governance.
Therefore, the policy challenge ahead is not to retreat into notions of cultural purity, but to govern openness with clarity and purpose. This requires strengthening integration frameworks and reinforcing institutional trust. It also requires recognising that engagement with other civilisational spaces is not a concession, but a necessity in a globally interconnected world.
In a world of intensifying geopolitical rivalry, it may be tempting to define strength in narrower terms. But doing so risks undertnining one of the West’s most important strategic assets. Openness — disciplined, governed, and anchored in strong institutions — is not a vulnerability. It is a source of sustained advantage.
(Milinda Moragoda –Former Sri Lankan Cabinet Minister, diplomat and the Founder of the Pathfinder Foundation, a strategic affairs think tank. The Hindu – 08, May 2026)
By Milinda Moragoda
Palm leaf manuscripts are now valued as historical documents and collections of palm leaf manuscripts are carefully preserved in libraries, in Sri Lanka and abroad. Most of the palm leaf manuscripts available in these collections date only from the 18th and 19th century. The palm leaf is a perishable item. Manuscripts of an earlier period are rare and are greatly valued.
Sri Lanka has the greatest number of these palm leaf manuscript collections. This indicates the value placed on palm leaf manuscripts in this country. The largest collection in Sri Lanka and possibly in the world, is in the National Museum Library, Colombo. The collection exceeds 5000. It includes the collections of H.C.P. Bell, W.A. de Silva, Ananda Coomaraswamy and E.B Gunaratne as well as the poetry section of the Hugh Neville collection. In 1938, W.A. de Silva prepared a “Catalogue of palm leaf manuscripts in the Library of the Colombo Museum.” This was published by the Museum.
The Museum library has the oldest palm leaf manuscript in the country, the Cullavagga, dated to 13 century. Cullavagga gives an account of the religious life of the sangha and the legal confines of their conduct. The last chapter carries the earliest known account of the Buddhist Great Council at Rajagaha.
The library has a copy of Buddhaghosa’s commentary on Digha nikaya. The cover is of silver embossed with white sapphires. The library has a copy of Sumangala Vilasini , one of the Bodhiwamsa (Ref No 1823) in Sinhala giving the history of the Sri Maha Bodhi, and the Mahavagga, copied by the Peramuna rala of Siyambalapitiya Galboda korale, completed on October 1802 and offered to Malwatte.
The Museum library has approximately 300 medical manuscripts Saddharmaratnavaliya manuscript says that doctors had to be paid for their services and travelling expenses. It said that physicians jealously guarded their knowledge of medicine and kept their prescriptions for medical remedies in safe custody.
University of Peradeniya has the next largest collection of 4000 items. Peradeniya has the UNESCO recognised copy of the Mahavamsa and the 13 century Visuddhi Magga Tika. The library has the de Saram and Hettiarachchy collections and several collections of palm leaf manuscripts donated to it.When I was studying at Peradeniya in the 1960s, the Main Library displayed palm leaf manuscripts and their decorative covers, in a case, upstairs, by the staircase, where the readers would not miss it. That was our introduction to palm leaf manuscripts.
The National Library of Sri Lanka (est. 1990) has a small but distinctive collection of 523 items which include Sinhala vedakam, Sinhala bana katha and Yantra mantra gurukam . It has a rare literary manuscript, Diya Savol Sandeshaya, dated April 26, 1904. It begins with the evocative phrase “Sarada Sarada Somi Paharusamu.” It provides a unique glimpse into the late-modern period of Sinhala literature. The manuscript is in good condition, with beginning and end intact. It measures 50 cm in length.
Other state institutes also have collections. The Institute of Indigenous Medicine, Rajagiriya has 700 palm leaf manuscripts. The collection includes Besajja Manjusa , the oldest medical manuscript in Sri Lanka . The collection also has a very old, valuable manuscript on acupuncture, written in Sinhala. The manuscript is reproduced in full in the book “Palm leaf manuscripts of Sri Lanka” by Sirancee Gunawardana. She comments, it is well illustrated. The human form is drawn clearly and acupuncture points indicated.
There are valuable private collections of palm leaf manuscripts, acquired by knowledgeable collectors. University of Kelaniya has digitised and made available the manuscripts of 13 private collections. The Danton Obeyesekera collection includes an ath-veda-pota containing prescriptions. James D Alwis collection has a copy of the Jataka Atuwa getapadaya. L.S.D Pieris has an extensive collection of Yantra manuscripts and medical manuscripts as well as a copy of the Rajavaliya. It was noted that SWRD Bandaranaike also had a collection of palm leaf manuscripts .
Private collectors seem to have been specially interested in the pansiya panas jataka. K.V.J. de Silva’s collection had a magnificent pansiya panas jataka. The collection assembled by Rohan de Silva and Jacques Soulie at the Suriyakantha Centre for Art & Culture, Handessa, also has on display a palm leaf manuscript of the Jataka stories, dated to late Kandyan period, in exceptional condition. Its clarity of script, leaf preparation, and intact binding show the highest standards of Sri Lankan scribal craftsmanship, the Centre said.
The largest collection in a foreign library (western) is probably the collection in the British Library, London, which has around 2464 Sinhala palm leaf manuscripts . The major portion of this collection is the Hugh Neville collection of 2227 palm leaf manuscripts. Everybody has heard of the Hugh Neville collection and most think that this is the only collection of Sri Lanka palm leaf manuscripts in the world and that we must be grateful to Hugh Neville for collecting them. Some probably think he wrote them. They do not know of the much larger collections in Colombo and Peradeniya.
Hugh Neville (1869 – 1886) came to Sri Lanka during the British period as private secretary to the Chief Justice. He later became an Assistant Government Agent. He travelled across the country collecting palm leaf manuscripts. They were mainly 19 century manuscripts. Hugh Nevill observed that just one in his collection may be 100 years old. I have no copy over 200 years old, he said.[1]
Hugh Neville died in France, but London acquired the palm leaf collection at the instigation of D.M de Z. Wickremasinghe. They were catalogued by K.D. Somadasa and published in seven volumes, titled ‘Catalogue of the Hugh Nevill Collection of Sinhalese manuscripts in the British Library”. The British Library, in 2021, digitized and made freely available online, four Sinhalese palm leaf manuscripts from the Hugh Nevill collections, namely Dighanikaya, Majjhimanikaya and two copies of Mahavamsa.
The libraries of Cambridge and Oxford Universities have Sri Lanka palm leaf manuscripts. Bodleian Library in Oxford has the Mahavamsa manuscript which was used by Turner for his English translation. Jinadasa Liyanaratana has examined some of the manuscripts in Cambridge and has catagloued 24 Sinhala manuscripts of which 6 were medical texts, others were on Buddhism. This was published in Journal of the Pali Text Society, Vol. XVIII, 1993, pp. 131-47[2]
The John Rylands Library, University of Manchester holds over seventy manuscripts from Sri Lanka, “mostly on Theravada in the Pali language in Sinhalese script” . They are probably from the Rhys Davids collection. The manuscripts date from the 17th-19th centuries and include copies made in Sri Lanka for T.W. Rhys Davis. There are complete manuscripts of the Paṭṭhāna-Pakaraṇa and Nettipakaraṇa, which are rare even in Sri Lanka.
There are palm leaf manuscripts at Bibliothèque Nationale, Paris, the Azistische Kjust Museum, Amsterdam, and Bavarian State Library in Munich . Paris has the Talapata sent from the Udarata chiefs to Dutch governor Falck. Jinadasa Liyanaratne examined and wrote on the “Sinhalese Medical Manuscripts in Paris” for Bulletin de l’École française d’Extrême-Orient Année 1987 pp. 185-199[3] The Netherlands collection included 135 medical manuscripts.
The palm leaf manuscript collection in the Royal Library, Copenhagen is well known. It was obtained by Rasmus Rask who came to Sri Lanka in 1822 in search of them. The collection was catalogued by C.E. Godakumbure. The catalogue is available in Gunawardene’s “Palm leaf manuscripts of Sri Lanka”(p 339). This collection contains the manuscripts collected by Ven. Kapugama Dharmachandra who lived in Dadalla, Galle. He converted to Christianity and his extensive collection, went to Denmark, said Gunawardana.[4]
Small collections of palm leaf manuscripts are held in various other foreign libraries in the west. Casey Wood, (b 1856) an American ophthalmologist who had in interest in medical research, toured the world after retirement. In Sri Lanka he connected with Andreas Nell, also an eye surgeon, obtained palm leaf manuscripts, mainly medical, which he then donated to institutions and individuals all over North America. At least 50 different recipients have been identified.[5]McGill University has a collection of 27 palm leaf manuscripts gifted by him.[6] The Metropolitan Museum of Art, in New York has one manuscript on display[7]. (To be continued)
[1] Stephne C Berkwitz. Buddhist history in the vernacular. P . 115..
[2] https://hasp.ub.uni-heidelberg.de/journals/jpts/article/view/28096/27490
[3] https://www.persee.fr/doc/befeo_0336-1519_1987_num_76_1_1723
[4] Sirancee Gunawardana Palm leaf manuscripts of Sri Lanka . (1977 )p 1-9, 35,41-43,50,127,129,140-146,248,286-292,339-,
[5] https://findingaids.library.northwestern.edu/repositories/8/resources/1303
[6] https://hiddenhands.ca/sri-lanka-essays/
[7] ps://libmma.contentdm.oclc.org/digital/collection/p16028coll4/id/47247/.
by KAMALIKA PIERIS

Britain’s Health Secretary Streeting resigns as pressure on Starmer grows

National SME Strategy Framework 2026 is critical because it brings policy consistency and stability to the sector – PM

Giant new dinosaur identified from fossils in Thailand

Cuba says CIA chief visited Havana as energy crisis worsens

Showers about 150mm are likely at some places in the Western, Sabaragamuwa and North-western provinces and showers above 100mm are likely at some places in Galle and Matara districts

Tilak Varma, Shardul Thakur hand Punjab Kings fifth successive defeat

‘Dates have the highest sugar content to fight Coronavirus’

Sunday Island 27 December – Headlines

#SundayIsland 17th December – Headlines

Sunday Island – 28th March

Sunday Island Headlines – 21 March

Sunday Island – 21st February – Headlines
-

 News5 days ago
News5 days agoLanka Port City officials to meet investors in Dubai
-

 News2 days ago
News2 days agoEx-SriLankan CEO’s death: Controversy surrounds execution of bail bond
-

 News6 days ago
News6 days agoSLPP expresses concern over death of former SriLankan CEO
-

 News6 days ago
News6 days agoPolice inform Fort Magistrate’s Court of finding ex-CEO of SriLankan dead under suspicious circumstances
-

 Features3 days ago
Features3 days agoWhen University systems fail:Supreme Court’s landmark intervention in sexual harassment case
-
Features3 days ago
High Stakes in Pursuing corruption cases
-

 Midweek Review2 days ago
Midweek Review2 days agoA victory that can never be forgotten
-

 News6 days ago
News6 days agoPresident of Vietnam and delegation departs Sri Lanka