Opinion
Numbers behind different COVID-19 vaccines

By M. C. M. Iqbal
The vaccines against COVID-19, available today, are based on different strategies and come with different numbers to indicate their performance. Many of us wish to know if one vaccine is better than the other. Two concepts underlying the performance of the vaccines are efficacy and effectiveness. The Pfizer-BioNTech vaccine has an efficacy of 95 percent, the Moderna Vaccine is 94.5 percent and the Russian made Sputnik vaccine is over 90 percent. Does this mean some vaccines are better than the other? The short answer is no. All the approved vaccines are equally good. So, let us look at what these numbers mean.
These numbers refer to statistical calculations to interpret the results of vaccination trials conducted by the manufacturers of vaccines, following a prescribed format. The method of calculation was developed over 100 years ago by two statisticians, who published their results in the Proceedings of the Royal Society of Medicine in 1915. They, Major Greenwood (Major is his first name and not a military title) and Udny Yule, were tasked with interpreting the results of immunization of British soldiers against typhoid and cholera, who were fighting in different regions of Europe and Asia favourable to the development of cholera epidemics. In a paper stretching over 82 pages, the authors developed the theoretical and mathematical background for calculating the efficacy of vaccines.
This article seeks to explain to the lay reader what these numbers imply and to bring out the differences between efficacy and effectiveness of a vaccine.
Efficacy and effectiveness
At first sight these two terms appear to be synonyms. However, in the world of vaccines and medicine, these two terms are not the same. Efficacy of a vaccine is how it performs under ideal and controlled conditions in a clinical trial (see below). During clinical trials, the outcome of vaccination is compared between a group of vaccinated people and another group given an inactive form of the vaccine (called a placebo). The effectiveness of a vaccine is how the vaccine performs in the real world – that is after the vaccine is approved by the regulatory agencies and you and I are vaccinated.
The efficacy of a vaccine is measured by the manufacturers under ideal conditions in a clinical trial where criteria are specified for selecting and excluding volunteers. These criteria are usually age groups, gender, ethnicity, geographical location and socio-economic standing. If the criteria are specific, then the effects of the vaccine or drug would not be applicable across the population. For example, if the COVID-19 vaccines are not tested on children below 18 years, then the approved vaccine cannot be used on children.
The effectiveness of a drug or vaccine is a measure of how well the drug or vaccine performs in real life, in a diverse population: Fitness geeks and couch potatoes, housewives and nurses, and farmers and office workers. Effectiveness is of relevance to the medical community and healthcare authorities who are treating the patients. Thus, studies on effectiveness would look at to what extent the vaccine is beneficial to the patient to prevent infection.
One may ask, why not simply look at the effectiveness of the vaccine? This is because if the participants in an initial trial of the vaccine are not carefully controlled, then it is difficult to interpret the outcome of the trial. We have many characteristics, which can potentially interfere with the outcome of a trial testing a vaccine. The person volunteering for the trial could be young or old, pregnant or not, a marathon runner or an average person and smoker or non-smoker. Thus, the volunteers selected for the trials are very similar within their groups with many criteria to exclude persons who could confuse the results (for example, an unhealthy person with other diseases would be excluded).
Efficacy of a vaccine asks the question ‘Does the vaccine work under ideal conditions?’ On the other hand, a study on the effectiveness of the same vaccine asks the question ‘Does vaccination work in the real world?’
Clinical trials
Under normal circumstances, vaccines take many years of research and testing to be approved. The COVID-19 pandemic was unprecedented, and pharmaceutical companies embarked on a race against time to produce safe and effective vaccines. The genome of this coronavirus, which was discovered by Chinese scientists, in January 2020, was a major contribution to the development of the vaccines. At the moment there are 94 vaccines being tested on humans in clinical trials, 32 of which have reached the final stage of Phase 3 testing.
To obtain approval for a vaccine, the vaccine manufacturers go through a prescribed process to ensure that the vaccine is safe. All the countries have a national drug approval agency, who should approve the use of a drug or vaccine in that country. The Food and Drug Administration (FDA) in the United States is an important regulatory agency, which has stringent criteria to approve medicines and drugs. In Sri Lanka, it is the National Medicines Regulatory Authority. COVID-19 vaccines are also assessed and approved by the WHO.
Initially, the vaccine is tested on cells in the laboratory and then given to animals, usually mice or monkeys. After this, if the mice or monkeys are happy, human volunteers are recruited to conduct the clinical trials, which is done in three phases. In the first phase, the vaccine is tested on a small group of people to determine the safety, dosage and ability to stimulate our immune system. If this is confirmed, the vaccine then moves into the Phase 2 stage where the safety of the vaccine is tested on hundreds of people who are split into different groups. Once these trials are successful, the vaccine moves to the final Phase 3 trials. Here thousands of people are recruited as volunteers. For the Pfizer-BioNTech vaccine there were over 40,000 volunteers, above the age of 16, from different countries. This trial is more comprehensive, with the volunteers belonging to different age groups, physical fitness, ethnicities and geographical locations. The volunteers are divided into two groups. One group gets the real vaccine while the other group gets a fake vaccine or placebo (the syringe has just water). The volunteers would not know if he/she is getting the vaccine or a placebo and neither do the nurses and doctors giving the vaccine. This is called a double-blind clinical trial. Thus, no one knows, except those conducting the trial, who was vaccinated with what.
After some time, the volunteers, who fell sick with the coronavirus, are PCR tested to confirm if they are COVID-19 positive. The scientists will be on the lookout for any side effects of the vaccine; if they find any cause for concern the trial can be stopped temporarily to conduct investigations and remedy the problem. If the scientists are not satisfied, the trial would be abandoned. Once the results are in, the calculations are done, and all the details are submitted to the regulating authorities. The regulators would ask the manufacturers more questions and once they are satisfied, approval is given to manufacture and market the vaccine. To accelerate the process, such as now during the COVID-19 crises, Phase 1 and 2 may be combined and run in parallel.
Calculating efficacy
The calculations involved are quite simple once the data is collected. Let us assume that 50,000 volunteers were recruited for the vaccination trial. Half were given the vaccine and the other half a placebo. Let us assume that of the 25,000 who received the vaccine, 10 persons were infected, and of the other 25,000 who received the placebo, 200 were infected. Although the numbers of people infected are small, those in the placebo group are 20 times larger (see Table). The researchers are concerned with the relative risk between the groups. This is called the efficacy of the vaccine.
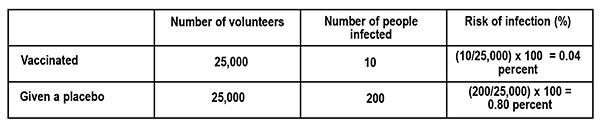
The risk of infection is calculated as follows.
What is the difference in the risk of infection between the vaccinated group and those who got the placebo? From the table this is, 0.80 percent – 0.04 percent = 0.76 percent.
Thus, the vaccine reduced the risk of infection by 0.76 percent, which looks quite small. This is what would happen if we are vaccinated. To understand this in terms of the risk of infection, if none were vaccinated, we look at the ratio of the Reduction in Infection (0.76 percent) to the Risk of infection (0.80 percent – those who got the fake vaccine). This is the Vaccine Efficacy (VE).
VE percent = Reduction in infection ÷ Risk of infection = 0.76 ÷ 0.80 = 95 percent
If this is still confusing, let us see what it means in a population of 100,000 persons who are vaccinated with a vaccine of 95 percent efficacy, and exposed to the virus. From the table above, the risk of infection for the vaccinated population is 0.04 percent, which translates to 40 persons (0.04 percent x 100,000). That is, we can expect that 40 persons would fall ill with an infection by the coronavirus and the rest of the vaccinated people may not develop an infection at all or develop an asymptomatic infection (you are infected but do not show symptoms) or get a mild disease.
(This example of calculating Vaccine Efficacy is adapted from an article by Dashiell Young-Saver in the New York Times of December 13, 2020, where the above calculation is explained in detail for students.)
What does efficacy mean?
The efficacy of a vaccine refers to two aspects. The first is how many of us are protected by the vaccine if we are exposed to the virus; this is given by the percentage. The vaccine also refers to different disease conditions it is capable of preventing. This could be causing an infection, mild disease, severe disease, hospitalisation, or death. This information can be found if one looks carefully at the statements issued by the vaccine manufacturer and regulatory agencies. For example, the statement by Pfizer-BioNTech states: Pfizer-BioNTech COVID-19 vaccine, BNT162b2, was 91.3 percent effective against COVID-19 (symptomatic cases of COVID-19), measured seven days through up to six months after the second dose. The vaccine was 100 percent effective against severe disease as defined by the US centres for Disease Control and Prevention (CDC), and 95.3 percent effective against severe disease as defined by the US FDA.
The efficacy of a vaccine (VE) is the relative reduction of being infected, if we are vaccinated, compared to the placebo or unvaccinated group. If the vaccine is perfect, then the risk of being infected is totally eliminated, so that VE = 1 or it is 100 percent. On the other hand, if there is no difference in the number of people infected between the two groups, the vaccine has no efficacy, or it is zero. Even with a perfect vaccine, our capacity to acquire an infection is determined by our age, health and immunity status.
In short, efficacy is a statistical measurement based on clinical trials of the vaccine’s ability to prevent infection. The volunteers taking part in the trials are not a perfect sample or representative of the real world (for example, children and sick people do not take part). Is there a lower limit for the efficacy of a vaccine to be accepted? Under the present circumstances, the FDA said it would consider granting emergency approval if the vaccines showed even 50 percent efficacy; the vaccines that have received approval now show an efficacy of over 90 percent.
Effectiveness
The effectiveness of the vaccine tells us how well the vaccine is performing among the population, in the real world, to prevent infection. The effectiveness of the vaccine depends on the impact it makes on society. After vaccination our immune system is primed to combat the coronavirus, reducing the multiplication of the virus in our body. This will gradually slow down the spread of the virus as more and more people are vaccinated. In other words, it is important that most if not all the people are vaccinated to have a large impact on the spread of the virus in society. Good examples are the smallpox vaccine, which completely eliminated the smallpox virus, and the polio vaccine, which has almost wiped out the polio virus except for a few small pockets in Pakistan, Afghanistan and Africa. Thus, the effectiveness of a vaccine looks at the medical and societal importance of the outcome.
Here is the above in a nutshell. The percentage numbers given with a vaccine refers to its efficacy – its ability to prevent an infection developing into a serious condition, determined under controlled clinical trials. Vaccines do not prevent infection – they prevent the infection from developing into a severe disease. Once we are vaccinated, our immune system is activated. If we are infected by the coronavirus, the virus has a small window of time to multiply, before it is eliminated by our immune system. This means we can release virus particles from our body, but much less than if we were not vaccinated. The message is we should get vaccinated with the first available vaccine and still wear our masks when going outside, even if we are vaccinated. The chances of ending up in a hospital is low and the chances of ending up in the ICU is very low. There is always a chance.
‘Tis impossible to be sure of anything but Death and Taxes (Christopher Bullock, 1716).
(M.C.M. Iqbal is Associate Research professor, Plant and Environmental Science, National Institute of Fundamental Studies, Hanthane Road, Kandy, and can be reached at iqbal.mo@nifs.ac.lk)
References
Zimmer, C. New York Times Nov. 20, 2020. Two companies say their vaccines are 95 percent effective. What does that mean?
Haelle,T. Association of Health Care Journalists. October 22, 2020. Know the nuances of vaccine efficacy when covering Covid-19 trials. https://healthjournalism.org/blog/2020/10/know-the-nuances-of-vaccine-efficacy-when-covering-covid-19-vaccine-trials/
Greenwood, M., & Yule, G. U. (1915). The Statistics of Anti-typhoid and Anti-cholera Inoculations, and the Interpretation of such Statistics in general. Proceedings of the Royal Society of Medicine, 8 (Sect Epidemiol State Med), 113–194.
Food and Drug Administration, US Department of Health and Human Services. https://www.fda.gov/media/139638/download

Children are the future of every nation, and the values they learn during childhood shape the society they will eventually lead. In Sri Lanka, where family traditions, respect for elders, and social responsibility have long been important cultural values, the way children are raised remains a topic of great interest. In recent years, many parents and educators have moved away from traditional forms of punishment and embraced more child-friendly approaches to discipline. While protecting children from physical and emotional harm is essential, an important question arises: can a child who grows up without any form of punishment or consequences become a threat to Sri Lankan society?
To answer this question, it is necessary to understand the difference between punishment and discipline. Punishment is often associated with penalties imposed for wrongdoing, while discipline refers to teaching children self-control, responsibility, and respect for rules. Modern child psychology generally discourages harsh physical punishment because it can cause fear, anxiety, and resentment. However, completely removing consequences for inappropriate behavior may create a different set of problems.
Sri Lankan society has traditionally emphasized discipline within the family. Parents, grandparents, and teachers have often played active roles in guiding children’s behavior. Respect for elders, obedience, and good manners have been considered important virtues. While some traditional disciplinary methods may no longer be acceptable, the underlying principle of teaching accountability remains relevant.
A child who never faces consequences for wrongdoing may struggle to understand the boundaries that exist in society. For example, if a child is allowed to insult others, damage property, or ignore rules without correction, they may develop the belief that their actions have no consequences. Such attitudes can become problematic when the child enters school, the workplace, or the wider community.
Sri Lankan schools already face challenges related to student discipline. Teachers often report difficulties in managing classrooms where some students refuse to follow instructions or respect school regulations. When children are not taught accountability at home, educational institutions may find it harder to maintain a productive learning environment. This can affect not only the individual student but also classmates whose education is disrupted.
Another concern is the development of entitlement. A child who is never told “no” may come to believe that personal desires should always be fulfilled. In a society where cooperation and mutual respect are essential, such attitudes can lead to conflicts with peers, teachers, employers, and even family members. Sri Lanka’s social fabric depends heavily on community relationships, and individuals who fail to respect others can weaken these bonds.
The influence of social media and modern technology has added another dimension to this issue. Today’s children have access to information and entertainment on an unprecedented scale. Without proper guidance and consequences, some may misuse technology, engage in cyberbullying, spread misinformation, or develop unhealthy habits. Parents who avoid setting limits may unintentionally expose children to risks that affect both personal development and social well-being.
The workplace offers another example of why accountability is important. Sri Lanka’s economic development depends on a workforce that is disciplined, responsible, and capable of working with others. Employers value punctuality, respect, and professionalism. Individuals who grow up without learning responsibility may find it difficult to meet these expectations, affecting both their personal success and the productivity of organizations.
However, it is equally important not to interpret this argument as support for harsh punishment. Research has shown that excessive physical or emotional punishment can have serious negative effects on children. Fear-based parenting may produce obedience in the short term but can damage confidence, trust, and mental health in the long term. Therefore, the solution is not stricter punishment but more effective discipline.
Positive discipline provides a balanced alternative. It involves setting clear rules, explaining expectations, and applying fair consequences when those rules are broken. For instance, if a child neglects schoolwork, they may lose certain privileges until responsibilities are fulfilled. If they damage property, they can be required to help repair or replace it. Such consequences teach accountability while preserving the child’s dignity.
Sri Lankan parents, teachers, and community leaders all have a role to play in nurturing responsible citizens. Families should create environments where children feel loved and supported but also understand that actions have consequences. Schools should encourage character development alongside academic achievement. Religious and community organizations can reinforce values such as honesty, compassion, and respect for others.
A balanced approach is especially important in a rapidly changing society. As Sri Lanka continues to modernize and integrate with the global community, young people must learn not only their rights but also their responsibilities. Freedom without responsibility can lead to selfishness, while discipline without compassion can lead to fear. The challenge is to find the middle ground.
A punishment-free child can become a concern for Sri Lankan society if the absence of punishment also means the absence of discipline and accountability. Children who never learn consequences may struggle to respect rules, authority, and the rights of others. However, harsh punishment is not the answer. The most effective approach combines love, guidance, clear boundaries, and fair consequences. By raising children who understand both freedom and responsibility, Sri Lanka can build a future generation that strengthens society rather than threatens it.
Saumya Aloysius
(An essayist, children’s writer and freelance writer who holds a Master’s Degree in Sociology from the University of Kelaniya)

On Friday 12 June, 2026, a SriLankan Airlines Airbus 330 was en route from Colombo to Sydney, Australia was about 45 minutes into its flight when a loud bang was heard, accompanied by a blinding flash. In what was assumed to be a lightning strike, the airplane’s left (No. 1) engine was damaged, forcing the aircraft to return to BIA-Katunayake, where it landed safely.
Lightning travels from cloud to cloud or cloud to ground. Because the aircraft is not electrically ‘grounded’, or ‘earthed’, it must have been in the path of the thunder bolt purely by chance. There is also a phenomenon whereby the aircraft may travel through an electrically charged atmosphere (for example a cloud) where an electrical charge could build up and strike, or be emitted, as lightning. In such an instance, pilots hear electrical static in their headsets before the strike. Usually, when lightning strikes an aircraft in flight, the electrical charges remain on the outside, as on a ‘Faraday’s Cage’ apparatus, and the passengers and crew are perfectly safe.
To help the efficient and safe discharge of static electricity from the airplane’s structure, static wicks, or static dischargers, are fitted at the trailing (rearmost) edges of the wings and tail surfaces. When an airplane has landed after a lightning strike, ground engineers count the number of wicks that may have been burnt out to ensure that a minimum (recommended) number is available for a subsequent flight. Sometimes, there is minor damage, like pitting of the paintwork at the points where the charges left the aircraft.
The last instance in the USA of an airplane believed to have been lost due to a lightning strike was on December 8, 1963, when a Pan Am Boeing 707-121, en route from Baltimore, Maryland to Philadelphia, Pennsylvania, suffered a fuel tank explosion, later determined to have been the result of a lightning strike. Since then, aircraft have been rendered immune from lightning damage thanks to extensive research conducted by manufacturers using high-voltage currents.
Interestingly, modern airliners have electronic instrument displays which don’t even flicker when the aircraft is struck by lightning. By a process of connecting all the metallic parts, known as ‘bonding’, the entire fuselage effectively becomes a protective cocoon, so electrical charges caused by lightning will always reside on the outside of the aircraft.
What is unusual in the recent SriLankan Airlines incident is the extent of damage to the left engine. Did it encounter hail or ingest something?
Only a thorough, independent inquiry by aviation safety investigators will reveal the cause.
GUWAN SEEYA

“Vision without execution is hallucination.” – Thomas Edison
Introduction: Stabilisation Is Not Transformation
Sri Lanka has come a long way since the economic collapse of 2022. Inflation has been brought under control. Foreign reserves have improved. Debt restructuring has advanced. Government revenue has increased significantly through taxation reforms. The exchange rate has stabilised, and confidence has gradually returned to financial markets.
These achievements deserve recognition.
However, stabilisation should not be confused with economic transformation. A patient discharged from intensive care is not necessarily healthy. Likewise, an economy that has escaped collapse has not necessarily achieved sustainable prosperity.
The central economic question facing Sri Lanka today is no longer how to avoid another crisis. Rather, it is how to achieve sustained economic growth of at least 7% per annum by 2029.
Unfortunately, much of the current policy debate remains trapped in economic diagnosis. Policymakers, economists, and commentators repeatedly identify familiar problems: (i) low productivity, (ii) weak exports, i(iii) Inadequate innovation, (iv) poor competitiveness, and (v) insufficient investment. While these diagnoses are correct, they are not new.
Sri Lanka now needs economic engineering.
The country requires a clear, measurable, and actionable National Growth Strategy for 2026-2029 that identifies (i) where growth will come from,(ii) what investments are required,(iii) which institutions will lead implementation, and (iv) how success will be measured.
The difference between diagnosis and engineering is the difference between describing a problem and solving it.
The Missing National Growth Target
One of the most striking weaknesses in Sri Lanka’s economic discourse is the absence of a publicly articulated growth target supported by a detailed implementation framework.
Successful economies establish measurable objectives.
Sri Lanka should adopt the following growth trajectory:
2026 – 4%
2027 – 5%
2028 – 6%
2029 – 7%
Such targets would provide direction to investors, public institutions, universities, exporters, and development partners. Without a destination, even the best policies risk becoming disconnected initiatives.
Today, many policy interventions appear fragmented—valuable in isolation but lacking integration into a broader national growth framework.
Growth Will Not Come From Consumption
For decades Sri Lanka relied heavily on consumption, imports, remittances, tourism, and external borrowing.
That model has reached its limits.
No country has achieved sustained prosperity through consumption-led growth alone.
The countries that transformed themselves—Singapore, South Korea, Ireland, Vietnam, and China—generated growth through productive investment, exports, industrialisation, and integration into global markets.
Sri Lanka’s future growth must therefore be driven by investment and exports rather than domestic consumption.
The challenge is not increasing spending but increasing productive capacity.
Export-Led Growth: The First Pillar of Transformation
Every successful Asian growth story has one characteristic in common: exports.
Exports generate foreign exchange, create jobs, attract investment, encourage innovation, and improve productivity.
Sri Lanka should establish an ambitious target of doubling export earnings within the next decade.
This requires moving beyond traditional exports and expanding into:
High-value agriculture
Food processing
Information technology services
Logistics services
Advanced manufacturing
Professional services
Export growth must become a national mission comparable to post-war reconstruction efforts seen elsewhere in Asia.
Without a major expansion of exports, sustained 7% growth will remain elusive.
Manufacturing: The Forgotten Growth Engine
Manufacturing remains the single most important source of rapid economic transformation worldwide. Vietnam provides perhaps the best recent example.
Through (i) industrial zones, (ii) trade agreements, (iii) infrastructure development, and (iv) targeted investment attraction, Vietnam became deeply integrated into Asian production networks.
Sri Lanka possesses strategic advantages:
A prime Indian Ocean location
Strong port infrastructure
Educated labour force
Proximity to India
The country should establish specialised manufacturing clusters focusing on:
Electronics assembly
Medical devices
Processed food products
Boat building
Rubber-based products
Engineering components
Rather than attempting to compete with every country, Sri Lanka should specialise in selected niches where competitive advantages can be developed.
RCEP: The Strategic Door to Asia
Sri Lanka’s future lies increasingly in Asia.
The Regional Comprehensive Economic Partnership (RCEP) represents the largest trading bloc in the world and includes many of the fastest-growing economies.
Membership or closer integration with RCEP supply chains could provide Sri Lankan exporters with access to markets, investment, technology, and production networks that are currently beyond reach.
Unfortunately, discussion on RCEP remains limited compared with its strategic significance.
A dedicated national roadmap for RCEP engagement should become a top economic priority.
The question is not whether Sri Lanka can afford to integrate more deeply into Asia.
The question is whether Sri Lanka can afford not to.
Knowledge Economy: Turning Universities Into Growth Institutions
Sri Lanka’s universities produce thousands of graduates annually, yet their contribution to commercial innovation remains limited.
Globally, universities have become engines of economic development.
Research institutions should not merely produce graduates; they should produce patents, technologies, startups, and commercial solutions.
A national innovation framework should:
Link universities with industry
Encourage commercialisation of research
Support technology transfer
Expand startup financing
Reward innovation and entrepreneurship
Knowledge must become an economic asset rather than an academic exercise.
Dairy, Agriculture, And Import Substitution
Export growth alone is insufficient.
Sri Lanka must also reduce unnecessary import dependence.
The dairy sector offers a compelling example.
For decades, billions of rupees have left the country through dairy imports despite favourable climatic conditions and substantial agricultural potential.
A comprehensive dairy development strategy should focus on:
Improved genetics
Feed production
Commercial farming
Processing investment
Farmer productivity
The objective should be import substitution combined with rural income growth.
The same principle can be applied selectively to other sectors where domestic production is economically viable.
Creating A National Investment Targeting Agency
Sri Lanka does not need another bureaucracy.
It needs a professional institution dedicated exclusively to investment targeting.
Instead of passively waiting for investors, this agency would actively identify and attract strategic investments aligned with national priorities.
Its mandate would include:
Identifying priority sectors
Marketing opportunities globally
Coordinating approvals
Monitoring outcomes
Facilitating technology transfer
Singapore’s Economic Development Board and Ireland’s Industrial Development Agency demonstrate how targeted investment institutions can transform national economies.
Sri Lanka requires a similar mechanism adapted to local realities.
From Economic Diagnosis To Economic Engineering
The next stage of Sri Lanka’s recovery requires a fundamental shift in thinking.
The policy debate must move beyond identifying problems. The country already knows its problems.The challenge is implementation.Every policy proposal should be evaluated against a simple question:
Will this contribute to achieving 7% growth by 2029?
If the answer is no, resources should be redirected.
Economic engineering requires focus, prioritisation, accountability, and measurable outcomes. The era of fragmented initiatives must give way to a coherent national growth strategy.
Summary
Sri Lanka has achieved significant macroeconomic stabilisation, but stabilisation is only the first step toward sustainable prosperity.
To move from recovery to transformation, Sri Lanka should adopt a National Growth Strategy for 2026-2029 built around five pillars:
Export-led growth
Investment-led growth
Manufacturing expansion
Knowledge-economy development
Regional integration through RCEP and Asian supply chains
Supporting sectors such as dairy, tourism, logistics, and information technology should be strategically developed within this framework.
Most importantly, investment must be targeted rather than scattered, supported by specialised institutions and measurable performance indicators.
Conclusion
History demonstrates that no nation has become prosperous by accident. Economic success is rarely the product of isolated policies or short-term political initiatives. It is the outcome of a deliberate strategy pursued consistently over many years.
Sri Lanka stands at a crossroads.
One path leads to modest growth, periodic crises, recurring debt challenges, and continued vulnerability. The other leads to transformation through investment, exports, innovation, manufacturing, and regional integration.
The choice is ultimately strategic.
The time has come for Sri Lanka to move from economic diagnosis to economic engineering.
The future will not be determined by how successfully the country stabilised after the crisis. It will be determined by how effectively it builds the foundations for sustained growth thereafter. If Sri Lanka can articulate and execute a coherent investment-led growth strategy today, achieving 7% growth by 2029 need not be an aspiration.
It can become a national objective—and a national achievement, economic Engineering
The writer, among many, served as the Special Advisor to the Office of the President of Namibia from 2006 to 2012 and was a Senior Consultant with the UNDP for 20 years. He was a Senior Economist with the Central Bank of Sri Lanka (1972-1993). He can be reached via asoka.seneviratne@gmail.com

FFSL renews National Team Head Coach Abdullah Almutairi under “The Next Chapter” program

Gakpo, Brobbey doubles give Dutch 5–1 World Cup win

Trump vows Iran will not charge Strait of Hormuz tolls, but says US might

Showers will occur in the Western, Sabaragamuwa and North-western provinces and in Galle, Matara, Kandy and Nuwara-Eliya districts

Govt. seeks INTERPOL assistance to bring Basil Rajapaksa back

Ravi warns against attempts to stir communal tensions over Easter attacks probe

‘Dates have the highest sugar content to fight Coronavirus’

Sunday Island 27 December – Headlines

#SundayIsland 17th December – Headlines

Sunday Island – 28th March

Sunday Island Headlines – 21 March

Sunday Island – 21st February – Headlines
-

 News6 days ago
News6 days agoRelease of 2025 O/L results likely to be delayed
-

 Sports6 days ago
Sports6 days agoTharanga set for high-profile javelin clash in Ostrava
-

 News6 days ago
News6 days agoTheft of USD 2.5 mn from Treasury: CoPF accused of complicity in NPP cover-up
-

 News5 days ago
News5 days agoBeijing Capital Airlines to resume flights to Colombo signalling boost to tourism
-

 Features4 days ago
Features4 days agoKilling of Colombo’s ancient trees — a warning on UN’s World Desertification Day – 17 June
-

 Opinion6 days ago
Opinion6 days agoDecoding Trump’s 12.5% “Forced Labor Tariff” on Sri Lanka
-

 Opinion6 days ago
Opinion6 days agoPalm leaf manuscripts of Sri Lanka – Part V
-

 News1 day ago
News1 day agoCreditor not yet paid