Features
Medical negligence or medical error ?
By Prof. Susirith Mendis
Preamble
The newspapers and social media have been full of news during the last few weeks about incidents in hospitals, which led to the death of patients. Obviously, we are aware of such incidents more now than then due to the feverish activity of social media.
The latest was the untimely and unnecessary death of Chamodi Sandeepani, a 21 year-old girl in the Teaching Hospital, Peradeniya. According to the mother of Chamodi, her daughter’s condition deteriorated and her body turned blue after the administration of two medications by a nurse. One of them had been identified as Ceftriaxone (a Cephalosporine antibiotic).
I was also truly disturbed when a very good friend of mine, a consultant anaesthesiologist – a long-time resident of UK, lost his brother, who was a card-carrying patient on his sensitivity to penicillin. He was injected with ‘Augementin’ (a combination drug of amoxicillin and clavulanic acid) in a major private hospital in Colombo and died immediately afterwards. It was alleged that the emergency tray was not readily available at the time of injection. There was hardly a ripple in the media about this incident.
Both these incidents point to anaphylactic shock. Death by anaphylactic shock occurs in all parts of the world – including the best of centres. But that does not mean that many of those were necessarily fatal. Some patients could have been revived with immediate appropriate response and emergency care. Too many incidents have been exposed in recent times about unexpected and untimely deaths of patients in hospitals. Allegations of negligence abound. These incidents must be investigated by independent investigators to ascertain the facts of each of these cases. The manner in which inquiries have been done in the past by the Ministry of Health leaves much to be desired. Most often, the end result is absolving the medical/health professionals and issues swept under the carpet. As in this case of Chamodi, where the inquiry panel is headed none other than by the DGHS – ‘a home and home affair’.
Nonetheless, as a medical professional, a medical teacher for over 40 years and a medical ethicist of some standing within and without our profession, I am most troubled by the responses and reactions I see in social media posted by doctors. There is a uniform response of criticising the victims and a myriad of excuses. There is not even a remote consideration of whether there has been negligence on the part of the medical/health professionals directly involved in the incident. There was a very recent case where a daughter who posted a bitter experience she had at the Nagoda Hospital of indifference and lack of concern and care in a facebook post. She was hounded and harassed by the police on a complaint from the hospital authorities. She was coerced by the Police to delete her post. A case of the combined effect of medical and police muscle.
A more conciliatory and introspective approach by the doctors will in the log run be more fruitful in improving the quality and standards of healthcare in the hospitals. Exuding arrogance, intimidatory self-defence and a mindset of ‘attack is the best form of defence’ is without doubt, counterproductive.My objective in this article is to look at the issues of medical negligence and medical errors in general and how they pertain to our perspective of the recent events that have taken hold of our attention during the last few weeks.
What I will not delve into in this article are the existent economic crisis that has lead to shortage of drugs, inferior drugs imported without due diligence to quality and standards, short-circuiting the due process and regulatory oversight of the National Medicines Regulatory Authority (NMRA) and the role played by the Minister of Health and the Ministry of Health. The last, but importantly, ‘clinician burnout’ due to the difficulties faced by medical and health professionals struggling to provide minimal patient care under dismal supply conditions. Collectively or singularly all of the above have directly or indirectly been responsible for these unfortunate deaths.
My comments herein, are issues related to medical negligence and medical error that are systemic as well as global.Let me start with a comment in a book that happened to catch my eye at the University of Georgetown Medical School Medical Ethics Library over 2 decades ago:
The book was “Examining your doctor: A patient’s guide to avoiding harmful medical care.” by Timothy B. McCall, MD (Carol Publishing Group, New York, 1995). This is the personal experience/confession of a doctor when he was training as a medical student in a University Hospital in te USA.
“My first experience taking care of patients as a medical student changed forever the way I viewed doctors. I was appalled. In the university hospital I was assigned, we treated one patient after another transferred from hospitals where they had received medical care that had nearly killed them. We saved some of them, though many of those we saved ended up disabled. We didn’t tell these patients or their families that they had been victims of poor medical care; we intentionally misled them. Covering up malpractice is just one example of the systematic way that doctors withhold information from their patients.”
Well, that says many things that most doctors in Sri Lanka would refuse to accept or even consider. Their arrogance ensures that they are never wrong. They can ever be wrong.
But, it is ironical that with better technology in healthcare available today, even in Sri Lanka, doctors are more likely to be found negligent. Is this because (i) medical standards have deteriorated? (ii) more doctors are now less skillful? (iii) they are now more careless? (iv) lawyers have realised that there is good money to make from ligigation against doctors? (v) patients have become more aware of their conditions (thanks to the internet) and therefore, more litigious? (vi) Insurance companies are paying good compensation? Or is it a relative permutation and combination of all of the above? I have not seen any serious scientific study done to ascertain the real situation in our country.
Let us now, look at a non-binding classification.
Medcal Negligence
It is an act of commission or omission by a healthcare provider in which care provided deviates from accepted standards of practice in the medical community and causes injury or death to the patient. To establish negligence, it is necessary to first establsih ‘duty of care’. A reasonable, foreseeable and actual loss or injury caused by or materially contributed to by a breach of duty of care will lead to an accusation of negligence.
This can be of two basic types: Criminal Negligence and Medical (or Clinical) Negligence. Criminal negligence is such that the negligence is grave enough for a police investigation and a prosecution by the Attorney General. It can lead to judicial sentencing and even imprisonment. Medical negligence, on the other hand, is a civil procedure, that could lead to damages being awarded by a Court of Law.
But prior to legal measures in a Court of Law, it is possible to pursue a lesser path of ‘pre-litigation’. This entails a departmental inquiry (Ministry of Health) which can lead from warning, transfer, punishment, reporting the the Sri Lanka Medical Council (SLMC) to even dismissal from service. A complaint to the SLMC can lead to periods of temporary suspension of registration. And in extreme instances, to complete erasure from the Medical Register.
There are even less serious avenues in instances where pateinet or their next of kin, can seek redress through a process of ‘conflict resolution’. Mediation is one of them. It has to be a voluntary process. There cannot be coercion on either parties – i.e., the doctors concerned or the patient. The parties meet privately with a neutral mediator who facilitates a negotiated agreement. This then binds the parties to that mutualyy agreed conditions of resolution of the conflict. This could be an unqualified apology to a meagre financial compensation for losses incurred. It is seen as a much more constructive and less adversarial process than conventional litigation. If agreement is not reached, the parties are free to initiate or continue with litigation.
Another non-litigious option for patients is to make a formal complaint to the Parliamentary Commissioner for Administration (better known as the Ombudsman). The present Ombudsman is a former Judge of the High Court of Sri Lanka. The former Secretary-General of Parliament, Sam Wijesinghe was the first – if my memory serves me right.
The positives of a non-litigious process is that it is (i) a non-threatening environment; (ii) it may give an increased sense of ‘fairness’ and justice for doctors; (iii) the legal and other costs are minimal and affordable to most.
The negatives are: (i) Will it give justice to the grievances of patients or their next of kin? (ii) Will the whole process be transparent and devoid of obvious bias? (iii) Will the process retain the confidence of both patients and doctors that justice has been done?
To ensure that the process is transparent and devoid of bias, there would be a need for non-medical or legal representation. Would it not be ideal, as in the Court process of ‘trial by a jury’, to have a committee of inquiry made up of competent civilians?
We, in Sri Lanka have no estimates of negligence. But, if we go by the many anecdotes of serious events of gross negligence we hear, and the number of litigation that have failed in a court f law or settled out of court, they are still a matter of very serious concern.
There are other conditions that I will not dwell at any length here. That is ‘medical misadventure’ where there is error or unexpected outcome during medical intervention leading to serious deleterious effect on patient. This happends most often in surgical and anaesthetic practice. An ‘adverse event’ is defined as an undesirable and unintentional, though not necessarily unexpected, result of medical treatment. Examples of an adverse event is discomfort in an artificial joint that continues after the expected recovery period, painful cheloids developing after open-heart surgery or a chronic headache following a spinal tap.
Medical Error
Medical error has been defined as an unintended act (either of omission or commission) or one that does not achieve its intended outcome; the failure of a planned action to be completed as intended (an error of execution); the use of a wrong plan to achieve an aim (an error of planning); or a deviation from the process of care that may or may not cause harm to the patient. Patient harm from medical error can occur at the individual or system level.
There are many ways that medical care can go wrong. Errors can occur around the administration of medications (including adverse drug events/reactions), during laboratory testing, pathology reports, hospital infections, as a result of surgery or even in documentation or data entry tasks.
Medication error are the leading cause of negligence, error and adverse events. They include; (i) prescribing errors; (ii) failure to prescribe, administer, or dispense a medication; (iii) a patient receiving a medication too late or too early; (iv) a patient receiving a drug not authorized for them; (v) improper use of a medication; (vi) wrong dose prescription or preparation; (vii) administration errors; (viii) failure to take into account a patient’s medical conditions or potential drug interactions; and (ix) not following proper dispensing/prescribing rules for a medication.
“To err is human”
An average of 195,000 people in the USA died due to potentially preventable, in-hospital medical errors in each of the years 2000, 2001 and 2002, according to a study of 37 million patient records. (The Health Grades Patient Safety in American Hospitals study (2000-02).
According to Dr. Lucien Leape, lead the author of a Harvard study, the number of deaths from medical errors in hospitals account for the equivalent to the death toll from three jumbo jet crashes every two days.( Public Health Reports , 1999; 114: 302-317 July/August, 1999).More people die each year in the United States from medical errors than from highway accidents, breast cancer or AIDS, a federal advisory panel has reported.
The report from the National Academy of Sciences’ Institute of Medicine cited studies showing between 44,000 and 98,000 people die each year because of mistakes by medical professionals. “That’s probably an underestimate for two reasons, one is, there are many different kinds of errors we never learn about — even in retrospective studies — because they are never written down. Second, these studies did not include other areas of care like home care, nursing homes and ambulatory care centers.” (Dr. Donald Berwick of the National Academic of Medicine, Washington DC). Medical error is the third leading cause of death in the US according to a BMJ article (BMJ 2016;353:i2139).
Here are some more statistics from the USA. The FDA receives more than 100,000 reports every year that are associated with medication errors (FDA, 2019). Forty-one percent of Americans report having been involved with a medical error either personally or secondhand (Institute for Healthcare Improvement/NORC at the University of Chicago, 2017). More than 7 million patients in the U.S. are impacted by medication errors every year (Journal of Community Hospital Internal Medicine Perspectives, 2016). Ten percent of hospital patients will be subject to a medication error (NCBI, 2019).By 2023, medication errors in the US has been tied to $40 billion in spending and up to 9000 deaths each year.
What about Sri Lanka?
To my knowledge, there are neither records of ‘medical error’ nor surveys or audits done for us to have an understanding, or even estimates, of medical negligence or errors in Sri Lanka. I am open to correction, if there are. The only record I know of is Professor Carlo Fonseka’s seminal article in the BMJ (Volume 313 21-28 December 1996) titled “To Err was Fatal”. In it he writes of five fatal errors he made that caused the death of five patient. I think it is compulsory reading for all doctors who have not yet read it. In it he makes five important and profound observations: (i) All doctors are fallible; (ii) The natural reaction of doctors to errors is to hide them or to rationalise them away; (iii) It is unscientific and unethical to refuse to face our errors; (iv) There is no cathartic ritual in our profession to expiate the sense of guilt generated by our errors; (v) Since knowledge grows mainly by error recognition, facing our errors squarely is the path to medical wisdom.
As Prof. Carlo Fonseka stated, doctors are not infallible, no matter how much patients would like them to be. While doctors’ mistakes are not usually intentional, they are often preventable and typically occur when doctors fail to exercise the proper level of care and skill. Hence, it is not difficult to accept that doctor errors occur more frequently than patients realise. The recent events are the tip of the proverbial iceberg.
Unfortunately, when doctors’ mistakes do happen, the consequences can be disastrous – even fatal. In which direction should we in Sri Lanka tread? The path traced by the West? Or go back to our own traditions and culture? Our social relations are based on the ‘Eastern Philosophical Tradition’. The Sri Lankan social milieu is predominantly based on Buddhist Philosophy – ‘The Four Noble Truths’ and ‘The Eightfold Path’ and the values of Meththa, Karuna, Muditha and Upeksha.
We are ‘serendipitously’ placed. We are a nation where all 4 major religions are practiced. Do we need to follow or abide by the Western medical ethical tradition coming down from Aesclepius and Hippocrates ?
We practice Modern Western Scientific Medicine in a socio-cultural milieu seeped in ancient Eastern traditions. Can we take inspiration from those traditions and synthesise a ‘New Medical ethical tradition’ by bridging this philosophical divide?
Do we have both the creativity and the courage to do so? If we have, we can in all probability avoid the pitfalls that the practice of medicine has fallen in the West (and in particular, the USA).Let these recent unfortunate and possible unavoidable deaths open us as medical professionals to a more humane and humanistic approach to patient care in Sri Lanka.











iyadasa Advisor to the Ministry of Science & Technology and a Board of Directors of Sri Lanka Atomic Energy Regulatory Council A value chain management consultant to www.vivonta.lk
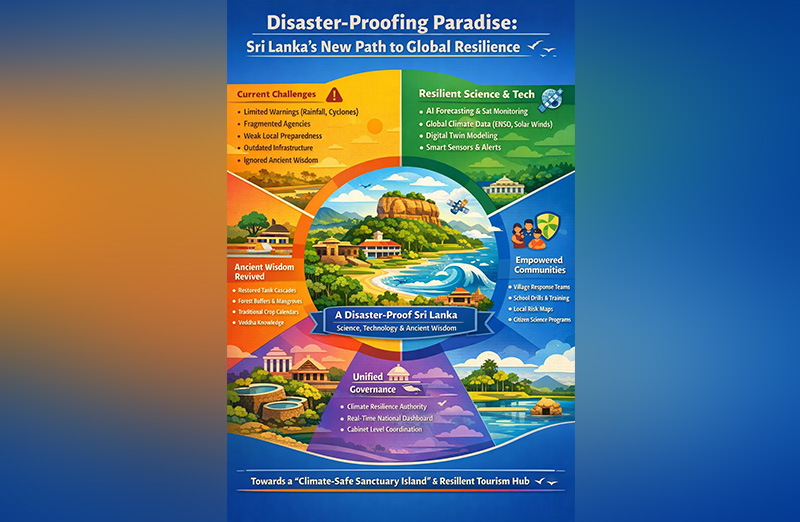
As climate shocks multiply worldwide from unseasonal droughts and flash floods to cyclones that now carry unpredictable fury Sri Lanka, long known for its lush biodiversity and heritage, stands at a crossroads. We can either remain locked in a reactive cycle of warnings and recovery, or boldly transform into the world’s first disaster-proof tropical nation — a secure haven for citizens and a trusted destination for global travelers.
The Presidential declaration to transition within one year from a limited, rainfall-and-cyclone-dependent warning system to a full-spectrum, science-enabled resilience model is not only historic — it’s urgent. This policy shift marks the beginning of a new era: one where nature, technology, ancient wisdom, and community preparedness work in harmony to protect every Sri Lankan village and every visiting tourist.
The Current System’s Fatal Gaps
Today, Sri Lanka’s disaster management system is dangerously underpowered for the accelerating climate era. Our primary reliance is on monsoon rainfall tracking and cyclone alerts — helpful, but inadequate in the face of multi-hazard threats such as flash floods, landslides, droughts, lightning storms, and urban inundation.
Institutions are fragmented; responsibilities crisscross between agencies, often with unclear mandates and slow decision cycles. Community-level preparedness is minimal — nearly half of households lack basic knowledge on what to do when a disaster strikes. Infrastructure in key regions is outdated, with urban drains, tank sluices, and bunds built for rainfall patterns of the 1960s, not today’s intense cloudbursts or sea-level rise.
Critically, Sri Lanka is not yet integrated with global planetary systems — solar winds, El Niño cycles, Indian Ocean Dipole shifts — despite clear evidence that these invisible climate forces shape our rainfall, storm intensity, and drought rhythms. Worse, we have lost touch with our ancestral systems of environmental management — from tank cascades to forest sanctuaries — that sustained this island for over two millennia.
This system, in short, is outdated, siloed, and reactive. And it must change.
A New Vision for Disaster-Proof Sri Lanka
Under the new policy shift, Sri Lanka will adopt a complete resilience architecture that transforms climate disaster prevention into a national development strategy. This system rests on five interlinked pillars:
Science and Predictive Intelligence
We will move beyond surface-level forecasting. A new national climate intelligence platform will integrate:
AI-driven pattern recognition of rainfall and flood events
Global data from solar activity, ocean oscillations (ENSO, MJO, IOD)
High-resolution digital twins of floodplains and cities
Real-time satellite feeds on cyclone trajectory and ocean heat
The adverse impacts of global warming—such as sea-level rise, the proliferation of pests and diseases affecting human health and food production, and the change of functionality of chlorophyll—must be systematically captured, rigorously analysed, and addressed through proactive, advance decision-making.
This fusion of local and global data will allow days to weeks of anticipatory action, rather than hours of late alerts.
Advanced Technology and Early Warning Infrastructure
Cell-broadcast alerts in all three national languages, expanded weather radar, flood-sensing drones, and tsunami-resilient siren networks will be deployed. Community-level sensors in key river basins and tanks will monitor and report in real-time. Infrastructure projects will now embed climate-risk metrics — from cyclone-proof buildings to sea-level-ready roads.
Governance Overhaul
A new centralised authority — Sri Lanka Climate & Earth Systems Resilience Authority — will consolidate environmental, meteorological, Geological, hydrological, and disaster functions. It will report directly to the Cabinet with a real-time national dashboard. District Disaster Units will be upgraded with GN-level digital coordination. Climate literacy will be declared a national priority.
People Power and Community Preparedness
We will train 25,000 village-level disaster wardens and first responders. Schools will run annual drills for floods, cyclones, tsunamis and landslides. Every community will map its local hazard zones and co-create its own resilience plan. A national climate citizenship programme will reward youth and civil organisations contributing to early warning systems, reforestation (riverbank, slopy land and catchment areas) , or tech solutions.
Reviving Ancient Ecological Wisdom
Sri Lanka’s ancestors engineered tank cascades that regulated floods, stored water, and cooled microclimates. Forest belts protected valleys; sacred groves were biodiversity reservoirs. This policy revives those systems:
Restoring 10,000 hectares of tank ecosystems
Conserving coastal mangroves and reintroducing stone spillways
Integrating traditional seasonal calendars with AI forecasts
Recognising Vedda knowledge of climate shifts as part of national risk strategy
Our past and future must align, or both will be lost.
A Global Destination for Resilient Tourism
Climate-conscious travelers increasingly seek safe, secure, and sustainable destinations. Under this policy, Sri Lanka will position itself as the world’s first “climate-safe sanctuary island” — a place where:
Resorts are cyclone- and tsunami-resilient
Tourists receive live hazard updates via mobile apps
World Heritage Sites are protected by environmental buffers
Visitors can witness tank restoration, ancient climate engineering, and modern AI in action
Sri Lanka will invite scientists, startups, and resilience investors to join our innovation ecosystem — building eco-tourism that’s disaster-proof by design.
Resilience as a National Identity
This shift is not just about floods or cyclones. It is about redefining our identity. To be Sri Lankan must mean to live in harmony with nature and to be ready for its changes. Our ancestors did it. The science now supports it. The time has come.
Let us turn Sri Lanka into the world’s first climate-resilient heritage island — where ancient wisdom meets cutting-edge science, and every citizen stands protected under one shield: a disaster-proof nation.

Why is national identity so important for a people? AI provides us with an answer worth understanding critically (Caveat: Even AI wisdom should be subjected to the Buddha’s advice to the young Kalamas):
‘A strong sense of identity is crucial for a people as it fosters belonging, builds self-worth, guides behaviour, and provides resilience, allowing individuals to feel connected, make meaningful choices aligned with their values, and maintain mental well-being even amidst societal changes or challenges, acting as a foundation for individual and collective strength. It defines “who we are” culturally and personally, driving shared narratives, pride, political action, and healthier relationships by grounding people in common values, traditions, and a sense of purpose.’
Ethnic Sinhalese who form about 75% of the Sri Lankan population have such a unique identity secured by the binding medium of their Buddhist faith. It is significant that 93% of them still remain Buddhist (according to 2024 statistics/wikipedia), professing Theravada Buddhism, after four and a half centuries of coercive Christianising European occupation that ended in 1948. The Sinhalese are a unique ancient island people with a 2500 year long recorded history, their own language and country, and their deeply evolved Buddhist cultural identity.
Buddhism can be defined, rather paradoxically, as a non-religious religion, an eminently practical ethical-philosophy based on mind cultivation, wisdom and universal compassion. It is an ethico-spiritual value system that prioritises human reason and unaided (i.e., unassisted by any divine or supernatural intervention) escape from suffering through self-realisation. Sri Lanka’s benignly dominant Buddhist socio-cultural background naturally allows unrestricted freedom of religion, belief or non-belief for all its citizens, and makes the country a safe spiritual haven for them. The island’s Buddha Sasana (Dispensation of the Buddha) is the inalienable civilisational treasure that our ancestors of two and a half millennia have bequeathed to us. It is this enduring basis of our identity as a nation which bestows on us the personal and societal benefits of inestimable value mentioned in the AI summary given at the beginning of this essay.
It was this inherent national identity that the Sri Lankan contestant at the 72nd Miss World 2025 pageant held in Hyderabad, India, in May last year, Anudi Gunasekera, proudly showcased before the world, during her initial self-introduction. She started off with a verse from the Dhammapada (a Pali Buddhist text), which she explained as meaning “Refrain from all evil and cultivate good”. She declared, “And I believe that’s my purpose in life”. Anudi also mentioned that Sri Lanka had gone through a lot “from conflicts to natural disasters, pandemics, economic crises….”, adding, “and yet, my people remain hopeful, strong, and resilient….”.
“Ayubowan! I am Anudi Gunasekera from Sri Lanka. It is with immense pride that I represent my Motherland, a nation of resilience, timeless beauty, and a proud history, Sri Lanka.
“I come from Anuradhapura, Sri Lanka’s first capital, and UNESCO World Heritage site, with its history and its legacy of sacred monuments and stupas…….”.
The “inspiring words” that Anudi quoted are from the Dhammapada (Verse 183), which runs, in English translation: “To avoid all evil/To cultivate good/and to cleanse one’s mind -/this is the teaching of the Buddhas”. That verse is so significant because it defines the basic ‘teaching of the Buddhas’ (i.e., Buddha Sasana; this is how Walpole Rahula Thera defines Buddha Sasana in his celebrated introduction to Buddhism ‘What the Buddha Taught’ first published in1959).
Twenty-five year old Anudi Gunasekera is an alumna of the University of Kelaniya, where she earned a bachelor’s degree in International Studies. She is planning to do a Master’s in the same field. Her ambition is to join the foreign service in Sri Lanka. Gen Z’er Anudi is already actively engaged in social service. The Saheli Foundation is her own initiative launched to address period poverty (i.e., lack of access to proper sanitation facilities, hygiene and health education, etc.) especially among women and post-puberty girls of low-income classes in rural and urban Sri Lanka.
Young Anudi is primarily inspired by her patriotic devotion to ‘my Motherland, a nation of resilience, timeless beauty, and a proud history, Sri Lanka’. In post-independence Sri Lanka, thousands of young men and women of her age have constantly dedicated themselves, oftentimes making the supreme sacrifice, motivated by a sense of national identity, by the thought ‘This is our beloved Motherland, these are our beloved people’.
The rescue and recovery of Sri Lanka from the evil aftermath of a decade of subversive ‘Aragalaya’ mayhem is waiting to be achieved, in every sphere of national engagement, including, for example, economics, communications, culture and politics, by the enlightened Anudi Gunasekeras and their male counterparts of the Gen Z, but not by the demented old stragglers lingering in the political arena listening to the unnerving rattle of “Time’s winged chariot hurrying near”, nor by the baila blaring monks at propaganda rallies.
Politically active monks (Buddhist bhikkhus) are only a handful out of the Maha Sangha (the general body of Buddhist bhikkhus) in Sri Lanka, who numbered just over 42,000 in 2024. The vast majority of monks spend their time quietly attending to their monastic duties. Buddhism upholds social and emotional virtues such as universal compassion, empathy, tolerance and forgiveness that protect a society from the evils of tribalism, religious bigotry and death-dealing religious piety.
Not all monks who express or promote political opinions should be censured. I choose to condemn only those few monks who abuse the yellow robe as a shield in their narrow partisan politics. I cannot bring myself to disapprove of the many socially active monks, who are articulating the genuine problems that the Buddha Sasana is facing today. The two bhikkhus who are the most despised monks in the commercial media these days are Galaboda-aththe Gnanasara and Ampitiye Sumanaratana Theras. They have a problem with their mood swings. They have long been whistleblowers trying to raise awareness respectively, about spreading religious fundamentalism, especially, violent Islamic Jihadism, in the country and about the vandalising of the Buddhist archaeological heritage sites of the north and east provinces. The two middle-aged monks (Gnanasara and Sumanaratana) belong to this respectable category. Though they are relentlessly attacked in the social media or hardly given any positive coverage of the service they are doing, they do nothing more than try to persuade the rulers to take appropriate action to resolve those problems while not trespassing on the rights of people of other faiths.
These monks have to rely on lay political leaders to do the needful, without themselves taking part in sectarian politics in the manner of ordinary members of the secular society. Their generally demonised social image is due, in my opinion, to three main reasons among others: 1) spreading misinformation and disinformation about them by those who do not like what they are saying and doing, 2) their own lack of verbal restraint, and 3) their being virtually abandoned to the wolves by the temporal and spiritual authorities.
(To be continued)
By Rohana R. Wasala ✍️

 ‘Adapt, shrink or die’ – thus runs the warning issued by the Trump administration to UN humanitarian agencies with brute insensitivity in the wake of its recent decision to drastically reduce to $2bn its humanitarian aid to the UN system. This is a substantial climb down from the $17bn the US usually provided to the UN for its humanitarian operations.
‘Adapt, shrink or die’ – thus runs the warning issued by the Trump administration to UN humanitarian agencies with brute insensitivity in the wake of its recent decision to drastically reduce to $2bn its humanitarian aid to the UN system. This is a substantial climb down from the $17bn the US usually provided to the UN for its humanitarian operations.
Considering that the US has hitherto been the UN’s biggest aid provider, it need hardly be said that the US decision would pose a daunting challenge to the UN’s humanitarian operations around the world. This would indeed mean that, among other things, people living in poverty and stifling material hardships, in particularly the Southern hemisphere, could dramatically increase. Coming on top of the US decision to bring to an end USAID operations, the poor of the world could be said to have been left to their devices as a consequence of these morally insensitive policy rethinks of the Trump administration.
Earlier, the UN had warned that it would be compelled to reduce its aid programs in the face of ‘the deepest funding cuts ever.’ In fact the UN is on record as requesting the world for $23bn for its 2026 aid operations.
If this UN appeal happens to go unheeded, the possibilities are that the UN would not be in a position to uphold the status it has hitherto held as the world’s foremost humanitarian aid provider. It would not be incorrect to state that a substantial part of the rationale for the UN’s existence could come in for questioning if its humanitarian identity is thus eroded.
Inherent in these developments is a challenge for those sections of the international community that wish to stand up and be counted as humanists and the ‘Conscience of the World.’ A responsibility is cast on them to not only keep the UN system going but to also ensure its increased efficiency as a humanitarian aid provider to particularly the poorest of the poor.
It is unfortunate that the US is increasingly opting for a position of international isolation. Such a policy position was adopted by it in the decades leading to World War Two and the consequences for the world as a result of this policy posture were most disquieting. For instance, it opened the door to the flourishing of dictatorial regimes in the West, such as that led by Adolph Hitler in Germany, which nearly paved the way for the subjugation of a good part of Europe by the Nazis.
If the US had not intervened militarily in the war on the side of the Allies, the West would have faced the distressing prospect of coming under the sway of the Nazis and as a result earned indefinite political and military repression. By entering World War Two the US helped to ward off these bleak outcomes and indeed helped the major democracies of Western Europe to hold their own and thrive against fascism and dictatorial rule.
Republican administrations in the US in particular have not proved the greatest defenders of democratic rule the world over, but by helping to keep the international power balance in favour of democracy and fundamental human rights they could keep under a tight leash fascism and linked anti-democratic forces even in contemporary times. Russia’s invasion and continued occupation of parts of Ukraine reminds us starkly that the democracy versus fascism battle is far from over.
Right now, the US needs to remain on the side of the rest of the West very firmly, lest fascism enjoys another unfettered lease of life through the absence of countervailing and substantial military and political power.
However, by reducing its financial support for the UN and backing away from sustaining its humanitarian programs the world over the US could be laying the ground work for an aggravation of poverty in the South in particular and its accompaniments, such as, political repression, runaway social discontent and anarchy.
What should not go unnoticed by the US is the fact that peace and social stability in the South and the flourishing of the same conditions in the global North are symbiotically linked, although not so apparent at first blush. For instance, if illegal migration from the South to the US is a major problem for the US today, it is because poor countries are not receiving development assistance from the UN system to the required degree. Such deprivation on the part of the South leads to aggravating social discontent in the latter and consequences such as illegal migratory movements from South to North.
Accordingly, it will be in the North’s best interests to ensure that the South is not deprived of sustained development assistance since the latter is an essential condition for social contentment and stable governance, which factors in turn would guard against the emergence of phenomena such as illegal migration.
Meanwhile, democratic sections of the rest of the world in particular need to consider it a matter of conscience to ensure the sustenance and flourishing of the UN system. To be sure, the UN system is considerably flawed but at present it could be called the most equitable and fair among international development organizations and the most far-flung one. Without it world poverty would have proved unmanageable along with the ills that come along with it.
Dehumanizing poverty is an indictment on humanity. It stands to reason that the world community should rally round the UN and ensure its survival lest the abomination which is poverty flourishes. In this undertaking the world needs to stand united. Ambiguities on this score could be self-defeating for the world community.
For example, all groupings of countries that could demonstrate economic muscle need to figure prominently in this initiative. One such grouping is BRICS. Inasmuch as the US and the West should shrug aside Realpolitik considerations in this enterprise, the same goes for organizations such as BRICS.
The arrival at the above international consensus would be greatly facilitated by stepped up dialogue among states on the continued importance of the UN system. Fresh efforts to speed-up UN reform would prove major catalysts in bringing about these positive changes as well. Also requiring to be shunned is the blind pursuit of narrow national interests.

Over 400,000 Russians killed, wounded for 0.8 percent of Ukraine in 2025

SCG curator ‘really happy’ with pitch for final Ashes Test

Showery condition is expected to enhance in the Eastern, Northern and Uva provinces during the coming days, due to the development of a low-level atmospheric disturbance to the East of Sri Lanka

GMOA warns of trade union action unless govt. urgently resolves critical issues in health sector

Elephant census urged as death toll nears 400

CTU raises questions about education reforms

‘Dates have the highest sugar content to fight Coronavirus’

Sunday Island 27 December – Headlines

#SundayIsland 17th December – Headlines

Sunday Island – 28th March

Sunday Island Headlines – 21 March

Sunday Island – 21st February – Headlines
-

 Sports4 days ago
Sports4 days agoGurusinha’s Boxing Day hundred celebrated in Melbourne
-

 News2 days ago
News2 days agoLeading the Nation’s Connectivity Recovery Amid Unprecedented Challenges
-

 Sports5 days ago
Sports5 days agoTime to close the Dickwella chapter
-

 Features3 days ago
Features3 days agoIt’s all over for Maxi Rozairo
-

 News5 days ago
News5 days agoEnvironmentalists warn Sri Lanka’s ecological safeguards are failing
-

 News3 days ago
News3 days agoDr. Bellana: “I was removed as NHSL Deputy Director for exposing Rs. 900 mn fraud”
-

 News2 days ago
News2 days agoDons on warpath over alleged undue interference in university governance
-

 Features5 days ago
Features5 days agoDigambaram draws a broad brush canvas of SL’s existing political situation