Opinion
Numbers behind different COVID-19 vaccines

By M. C. M. Iqbal
The vaccines against COVID-19, available today, are based on different strategies and come with different numbers to indicate their performance. Many of us wish to know if one vaccine is better than the other. Two concepts underlying the performance of the vaccines are efficacy and effectiveness. The Pfizer-BioNTech vaccine has an efficacy of 95 percent, the Moderna Vaccine is 94.5 percent and the Russian made Sputnik vaccine is over 90 percent. Does this mean some vaccines are better than the other? The short answer is no. All the approved vaccines are equally good. So, let us look at what these numbers mean.
These numbers refer to statistical calculations to interpret the results of vaccination trials conducted by the manufacturers of vaccines, following a prescribed format. The method of calculation was developed over 100 years ago by two statisticians, who published their results in the Proceedings of the Royal Society of Medicine in 1915. They, Major Greenwood (Major is his first name and not a military title) and Udny Yule, were tasked with interpreting the results of immunization of British soldiers against typhoid and cholera, who were fighting in different regions of Europe and Asia favourable to the development of cholera epidemics. In a paper stretching over 82 pages, the authors developed the theoretical and mathematical background for calculating the efficacy of vaccines.
This article seeks to explain to the lay reader what these numbers imply and to bring out the differences between efficacy and effectiveness of a vaccine.
Efficacy and effectiveness
At first sight these two terms appear to be synonyms. However, in the world of vaccines and medicine, these two terms are not the same. Efficacy of a vaccine is how it performs under ideal and controlled conditions in a clinical trial (see below). During clinical trials, the outcome of vaccination is compared between a group of vaccinated people and another group given an inactive form of the vaccine (called a placebo). The effectiveness of a vaccine is how the vaccine performs in the real world – that is after the vaccine is approved by the regulatory agencies and you and I are vaccinated.
The efficacy of a vaccine is measured by the manufacturers under ideal conditions in a clinical trial where criteria are specified for selecting and excluding volunteers. These criteria are usually age groups, gender, ethnicity, geographical location and socio-economic standing. If the criteria are specific, then the effects of the vaccine or drug would not be applicable across the population. For example, if the COVID-19 vaccines are not tested on children below 18 years, then the approved vaccine cannot be used on children.
The effectiveness of a drug or vaccine is a measure of how well the drug or vaccine performs in real life, in a diverse population: Fitness geeks and couch potatoes, housewives and nurses, and farmers and office workers. Effectiveness is of relevance to the medical community and healthcare authorities who are treating the patients. Thus, studies on effectiveness would look at to what extent the vaccine is beneficial to the patient to prevent infection.
One may ask, why not simply look at the effectiveness of the vaccine? This is because if the participants in an initial trial of the vaccine are not carefully controlled, then it is difficult to interpret the outcome of the trial. We have many characteristics, which can potentially interfere with the outcome of a trial testing a vaccine. The person volunteering for the trial could be young or old, pregnant or not, a marathon runner or an average person and smoker or non-smoker. Thus, the volunteers selected for the trials are very similar within their groups with many criteria to exclude persons who could confuse the results (for example, an unhealthy person with other diseases would be excluded).
Efficacy of a vaccine asks the question ‘Does the vaccine work under ideal conditions?’ On the other hand, a study on the effectiveness of the same vaccine asks the question ‘Does vaccination work in the real world?’
Clinical trials
Under normal circumstances, vaccines take many years of research and testing to be approved. The COVID-19 pandemic was unprecedented, and pharmaceutical companies embarked on a race against time to produce safe and effective vaccines. The genome of this coronavirus, which was discovered by Chinese scientists, in January 2020, was a major contribution to the development of the vaccines. At the moment there are 94 vaccines being tested on humans in clinical trials, 32 of which have reached the final stage of Phase 3 testing.
To obtain approval for a vaccine, the vaccine manufacturers go through a prescribed process to ensure that the vaccine is safe. All the countries have a national drug approval agency, who should approve the use of a drug or vaccine in that country. The Food and Drug Administration (FDA) in the United States is an important regulatory agency, which has stringent criteria to approve medicines and drugs. In Sri Lanka, it is the National Medicines Regulatory Authority. COVID-19 vaccines are also assessed and approved by the WHO.
Initially, the vaccine is tested on cells in the laboratory and then given to animals, usually mice or monkeys. After this, if the mice or monkeys are happy, human volunteers are recruited to conduct the clinical trials, which is done in three phases. In the first phase, the vaccine is tested on a small group of people to determine the safety, dosage and ability to stimulate our immune system. If this is confirmed, the vaccine then moves into the Phase 2 stage where the safety of the vaccine is tested on hundreds of people who are split into different groups. Once these trials are successful, the vaccine moves to the final Phase 3 trials. Here thousands of people are recruited as volunteers. For the Pfizer-BioNTech vaccine there were over 40,000 volunteers, above the age of 16, from different countries. This trial is more comprehensive, with the volunteers belonging to different age groups, physical fitness, ethnicities and geographical locations. The volunteers are divided into two groups. One group gets the real vaccine while the other group gets a fake vaccine or placebo (the syringe has just water). The volunteers would not know if he/she is getting the vaccine or a placebo and neither do the nurses and doctors giving the vaccine. This is called a double-blind clinical trial. Thus, no one knows, except those conducting the trial, who was vaccinated with what.
After some time, the volunteers, who fell sick with the coronavirus, are PCR tested to confirm if they are COVID-19 positive. The scientists will be on the lookout for any side effects of the vaccine; if they find any cause for concern the trial can be stopped temporarily to conduct investigations and remedy the problem. If the scientists are not satisfied, the trial would be abandoned. Once the results are in, the calculations are done, and all the details are submitted to the regulating authorities. The regulators would ask the manufacturers more questions and once they are satisfied, approval is given to manufacture and market the vaccine. To accelerate the process, such as now during the COVID-19 crises, Phase 1 and 2 may be combined and run in parallel.
Calculating efficacy
The calculations involved are quite simple once the data is collected. Let us assume that 50,000 volunteers were recruited for the vaccination trial. Half were given the vaccine and the other half a placebo. Let us assume that of the 25,000 who received the vaccine, 10 persons were infected, and of the other 25,000 who received the placebo, 200 were infected. Although the numbers of people infected are small, those in the placebo group are 20 times larger (see Table). The researchers are concerned with the relative risk between the groups. This is called the efficacy of the vaccine.
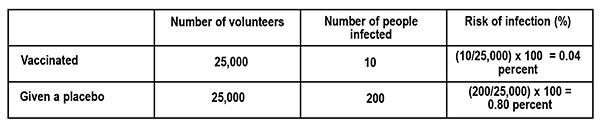
The risk of infection is calculated as follows.
What is the difference in the risk of infection between the vaccinated group and those who got the placebo? From the table this is, 0.80 percent – 0.04 percent = 0.76 percent.
Thus, the vaccine reduced the risk of infection by 0.76 percent, which looks quite small. This is what would happen if we are vaccinated. To understand this in terms of the risk of infection, if none were vaccinated, we look at the ratio of the Reduction in Infection (0.76 percent) to the Risk of infection (0.80 percent – those who got the fake vaccine). This is the Vaccine Efficacy (VE).
VE percent = Reduction in infection ÷ Risk of infection = 0.76 ÷ 0.80 = 95 percent
If this is still confusing, let us see what it means in a population of 100,000 persons who are vaccinated with a vaccine of 95 percent efficacy, and exposed to the virus. From the table above, the risk of infection for the vaccinated population is 0.04 percent, which translates to 40 persons (0.04 percent x 100,000). That is, we can expect that 40 persons would fall ill with an infection by the coronavirus and the rest of the vaccinated people may not develop an infection at all or develop an asymptomatic infection (you are infected but do not show symptoms) or get a mild disease.
(This example of calculating Vaccine Efficacy is adapted from an article by Dashiell Young-Saver in the New York Times of December 13, 2020, where the above calculation is explained in detail for students.)
What does efficacy mean?
The efficacy of a vaccine refers to two aspects. The first is how many of us are protected by the vaccine if we are exposed to the virus; this is given by the percentage. The vaccine also refers to different disease conditions it is capable of preventing. This could be causing an infection, mild disease, severe disease, hospitalisation, or death. This information can be found if one looks carefully at the statements issued by the vaccine manufacturer and regulatory agencies. For example, the statement by Pfizer-BioNTech states: Pfizer-BioNTech COVID-19 vaccine, BNT162b2, was 91.3 percent effective against COVID-19 (symptomatic cases of COVID-19), measured seven days through up to six months after the second dose. The vaccine was 100 percent effective against severe disease as defined by the US centres for Disease Control and Prevention (CDC), and 95.3 percent effective against severe disease as defined by the US FDA.
The efficacy of a vaccine (VE) is the relative reduction of being infected, if we are vaccinated, compared to the placebo or unvaccinated group. If the vaccine is perfect, then the risk of being infected is totally eliminated, so that VE = 1 or it is 100 percent. On the other hand, if there is no difference in the number of people infected between the two groups, the vaccine has no efficacy, or it is zero. Even with a perfect vaccine, our capacity to acquire an infection is determined by our age, health and immunity status.
In short, efficacy is a statistical measurement based on clinical trials of the vaccine’s ability to prevent infection. The volunteers taking part in the trials are not a perfect sample or representative of the real world (for example, children and sick people do not take part). Is there a lower limit for the efficacy of a vaccine to be accepted? Under the present circumstances, the FDA said it would consider granting emergency approval if the vaccines showed even 50 percent efficacy; the vaccines that have received approval now show an efficacy of over 90 percent.
Effectiveness
The effectiveness of the vaccine tells us how well the vaccine is performing among the population, in the real world, to prevent infection. The effectiveness of the vaccine depends on the impact it makes on society. After vaccination our immune system is primed to combat the coronavirus, reducing the multiplication of the virus in our body. This will gradually slow down the spread of the virus as more and more people are vaccinated. In other words, it is important that most if not all the people are vaccinated to have a large impact on the spread of the virus in society. Good examples are the smallpox vaccine, which completely eliminated the smallpox virus, and the polio vaccine, which has almost wiped out the polio virus except for a few small pockets in Pakistan, Afghanistan and Africa. Thus, the effectiveness of a vaccine looks at the medical and societal importance of the outcome.
Here is the above in a nutshell. The percentage numbers given with a vaccine refers to its efficacy – its ability to prevent an infection developing into a serious condition, determined under controlled clinical trials. Vaccines do not prevent infection – they prevent the infection from developing into a severe disease. Once we are vaccinated, our immune system is activated. If we are infected by the coronavirus, the virus has a small window of time to multiply, before it is eliminated by our immune system. This means we can release virus particles from our body, but much less than if we were not vaccinated. The message is we should get vaccinated with the first available vaccine and still wear our masks when going outside, even if we are vaccinated. The chances of ending up in a hospital is low and the chances of ending up in the ICU is very low. There is always a chance.
‘Tis impossible to be sure of anything but Death and Taxes (Christopher Bullock, 1716).
(M.C.M. Iqbal is Associate Research professor, Plant and Environmental Science, National Institute of Fundamental Studies, Hanthane Road, Kandy, and can be reached at iqbal.mo@nifs.ac.lk)
References
Zimmer, C. New York Times Nov. 20, 2020. Two companies say their vaccines are 95 percent effective. What does that mean?
Haelle,T. Association of Health Care Journalists. October 22, 2020. Know the nuances of vaccine efficacy when covering Covid-19 trials. https://healthjournalism.org/blog/2020/10/know-the-nuances-of-vaccine-efficacy-when-covering-covid-19-vaccine-trials/
Greenwood, M., & Yule, G. U. (1915). The Statistics of Anti-typhoid and Anti-cholera Inoculations, and the Interpretation of such Statistics in general. Proceedings of the Royal Society of Medicine, 8 (Sect Epidemiol State Med), 113–194.
Food and Drug Administration, US Department of Health and Human Services. https://www.fda.gov/media/139638/download
“As a small and open country, Singapore will always be vulnerable to what happens around us. As Lee Kuan Yew used to say: “when elephants fight, the grass suffers, but when elephants make love, the grass also suffers“. Therefore, we must be aware of what is happening around us, and prepare ourselves for changes and surprises.” – Prime Minister Lee Hsien Loong, during the debate on the President’s Address in Singapore Parliament on 16 May, 2018, commenting on the uncertain external environment during the first Trump Administration.
“When elephants fight, it is the grass that suffers”
is a well-known African proverb commonly used in geopolitics to describe smaller nations caught in the crossfire of conflicts between major powers. At the 1981 Commonwealth conference, when Tanzanian President Julius Nyerere quoted this Swahili proverb, the Prime Minister Lee Kuan Yew famously retorted, “When elephants make love, the grass suffers, too”. In other words, not only when big powers (such as the US, Russia, EU, China or India) clash, the surrounding “grass” (smaller nations) get “trampled” or suffer collateral damage but even when big powers collaborate or enter into friendly agreements, small nations can still be disadvantaged through unintended consequences of those deals. Since then, Singaporean leaders have often quoted this proverb to highlight the broader reality for smaller states, during great power rivalry and from their alliances. They did this to underline the need to prepare Singapore for challenges stemming from the uncertain external environment and to maintain high resilience against global crises.
Like Singapore, as a small and open country, Sri Lanka too is always vulnerable to what happens around us. Hence, we must be alert to what is happening around us, and be ready not only to face challenges but to explore opportunities.
When Elephants Fight
To begin with, President Trump’s “Operation Epic Fury”.
Did we prepare adequately for changes and surprises that could arise from the deteriorating situation in the Gulf region? For example, the impact the conflict has on the safety and welfare of Sri Lankans living in West Asia or on our petroleum and LNG imports. The situation in the Gulf remains fluid with potential for further escalation, with the possibility of a long-term conflict.
The region, which is the GCC, Iraq, Iran, Israel, Jordan, Syria and Azerbaijan (I believe exports to Azerbaijan are through Iran), accounts for slightly over $1 billion of our exports. The region is one of the most important markets for tea (US$546 million out of US$1,408 million in 2024. According to some estimates, this could even be higher). As we export mostly low-grown teas to these countries, the impact of the conflict on low-grown tea producers, who are mainly smallholders, would be extremely strong. Then there are other sectors like fruits and vegetables where the impact would be immediate, unless of course exporters manage to divert these perishable products to other markets. If the conflict continues for a few more weeks or months, managing these challenges will be a difficult task for the nation, not simply for the government. It is also necessary to remember the Russia – Ukraine war, now on to its fifth year, and its impact on Sri Lanka’s economy.
Mother of all bad timing
What is more unfortunate is that the Gulf conflict is occurring on top of an already intensifying global trade war. One observer called it the “mother of all bad timing”. The combination is deadly.
Early last year, when President Trump announced his intention to weaponise tariffs and use them as bargaining tools for his geopolitical goals, most observers anticipated that he would mainly use tariffs to limit imports from the countries with which the United States had large trade deficits: China, Mexico, Vietnam, the European Union, Japan and Canada. The main elephants, who export to the United States. But when reciprocal tariffs were declared on 2nd April, some of the highest reciprocal tariffs were on Saint Pierre and Miquelon (50%), a French territory off Canada with a population of 6000 people, and Lesotho (50%), one of the poorest countries in Southern Africa. Sri Lanka was hit with a 44% reciprocal tariff. In dollar terms, Sri Lanka’s goods trade deficit with the United States was very small (US$ 2.9 billion in 2025) when compared to those of China (US$ 295 billion in 2024) or Vietnam (US$ 123 billion in 2024).
Though the adverse impact of US additional ad valorem duty has substantially reduced due to the recent US Supreme Court decision on reciprocal tariffs, the turbulence in the US market would continue for the foreseeable future. The United States of America is the largest market for Sri Lanka and accounts for nearly 25% of our exports. Yet, Sri Lanka’s exports to the United States had remained almost stagnant (around the US $ 3 billion range) during the last ten years, due to the dilution of the competitive advantage of some of our main export products in that market. The continued instability in our largest market, where Sri Lanka is not very competitive, doesn’t bode well for Sri Lanka’s economy.
When Elephants Make Love
In rapidly shifting geopolitical environments, countries use proactive anticipatory diplomacy to minimise the adverse implications from possible disruptions and conflicts. Recently concluded Free Trade Agreement (FTA) negotiations between India and the EU (January 2026) and India and the UK (May 2025) are very good examples for such proactive diplomacy. These negotiations were formally launched in June 2007 and were on the back burner for many years. These were expedited as strategic responses to growing U.S. protectionism. Implementation of these agreements would commence during this year.
When negotiations for a free trade agreement between India and the European Union (which included the United Kingdom) were formally launched, anticipating far-reaching consequences of such an agreement on other developing countries, the Commonwealth Secretariat requested the University of Sussex to undertake a study on a possible implication of such an agreement on other low-income developing countries. The authors of that study had considered the impact of an EU–India Free Trade Agreement on the trade of excluded countries and had underlined, “The SAARC countries are, by a long way, the most vulnerable to negative impacts from the FTA. Their exports are more similar to India’s…. Bangladesh is most exposed in the EU market, followed by Pakistan and Sri Lanka.”
So, now these agreements are finalised; what will be the implications of these FTAs between India and the UK and the EU on Sri Lanka? According to available information, the FTA will be a game-changer for the Indian apparel exporters, as it would provide a nearly ten per cent tariff advantage to them. That would level the playing field for India, vis-à-vis their regional competitors. As a result, apparel exports from India to the UK and the EU are projected to increase significantly by 2030. As the sizes of the EU’s and the UK’s apparel markets are not going to expand proportionately, these growths need to come from the market shares of other main exporters like Sri Lanka.
So, “also, when elephants make love, the grass suffers.”
Impact on Sri Lanka
As a small, export dependent country with limited product and market diversification, Sri Lanka will always be vulnerable to what happens in our main markets. Therefore, we must be aware of what is happening in those markets, and prepare ourselves to face the challenges proactively. Today, amid intense geopolitical conflicts, tensions and tariff shifts, countries adopt high agility and strategic planning. If we look at what our neighbours have been doing in London, Brussels and Tokyo, we can learn some lessons on how to navigate through these turbulences.
(The writer is a retired public servant and can be reached at senadhiragomi@gmail.com)
by Gomi Senadhira

The introduction of the QR code–based fuel quota system can be seen as a timely and necessary measure, implemented as part of broader austerity efforts to manage limited fuel resources. In the face of ongoing global fuel instability and economic challenges, such a system is aimed at ensuring equitable distribution and preventing excessive consumption. While it is undeniable that this policy may disrupt the daily routines of certain segments of the population, it is important for citizens to recognize the larger national interest at stake and cooperate with these temporary measures until stability returns to the global fuel market.
At the same time, this initiative presents an important opportunity for the Government to address long-standing gaps in regulatory enforcement. In particular, the implementation of the QR code system could have been strategically linked to the issuance of valid revenue licenses for vehicles. Restricting QR code access only to vehicles that are properly registered and have paid their revenue dues would have helped strengthen compliance and improve state revenue collection.
Available data from the relevant authorities indicate that a significant number of vehicles—especially three-wheelers and motorcycles—continue to operate without valid revenue licences. This represents a substantial loss of income to the State and highlights a weakness in enforcement mechanisms. By integrating the fuel quota system with revenue license verification, the government could have effectively encouraged vehicle owners to regularise their documentation while simultaneously improving fiscal discipline.
In summary, while the QR code fuel system is a commendable step toward managing scarce resources, aligning it with existing regulatory requirements would have amplified its benefits. Such an approach would not only support fuel conservation but also enhance government revenue and promote greater accountability among vehicle owners.
Sariputhra
Colombo 05

First, let us see why the war started by Israel and the US against Iran may be seen as a stupid undertaking. Israel was aiming for regional hegemony and US world dominance, which could be called an utterly foolish dream in today’s multipolar world order, which the theatre of war now reveals. They may have underestimated Iran’s capacity and also the economic fallout due to its ability to control the Strait of Hormuz.
In February 2026, reports emerged that General Dan Caine, the U.S. Chairman of the Joint Chiefs of Staff, privately warned President Trump about the significant risks of a major war with Iran, including potential U.S. casualties, depleted ammunition stockpiles and entanglement in a prolonged conflict. However, President Trump publicly dismissed these reports as incorrect. General Caine’s appointment by President Trump was considered controversial, as Caine was chosen over many active-duty four-star generals and lacks experience as a combatant commander or service chief. Under these circumstances Caine would have been expected to be subservient to Trump, yet he opted to disagree as he saw the danger. Trump countered his arguments saying it would be a quick job, take out the leadership, destroy the military structure and the people will take over the country. This did not happen and now most of the scenarios that Caine said was possible are gradually coming true.
Israel suffers damage
For Israel, too, damage is much more than expected and could prove to be decisive in its expansionist ambitions in the region if not its very existence. It had previously tried to drag former US presidents, Bush, Obama and Biden into a war with Iran, but they were aware of the underlying danger. The Gulf countries too were hit hard and the US could not protect them, and they may be regretting that they ever let the US set up military bases on their soil. Former US secretary of state Henry Kissinger once famously said, “To be America’s enemy is dangerous, to be its friend is fatal”.
The US may have succeeded in making states, such as Iraq, Syria and Libya, fail, but Iran is a different kettle of fish. Trump was jubilant after capturing the Venezuelan president and may have been planning to lay his hands on Cuba and Turkey and then try to annex Canada and Greenland. A man who promised a “no war” policy in his presidential campaign has converted his department of defence into a department of war in the real sense of the term. Trump must realise that he cannot act like a global policeman and undermine the sovereignty of other nations with impunity. Trump says “we have won” but has nothing to show as gains in the Iran war.
Trump’s concern about BRICS
Another factor in the equation is that Trump may have been concerned about the growing influence and membership of BRICS, which in effect appears to be anti-American if one were to go by its attempt to de-dollarise world trade. Of particular concern may have been the recent admission into BRICS, of several countries supposed to be staunch US allies, such as Saudi Arabia, UAE, and Egypt. Iran is an active member and was mending its fences with Saudi Arabia under the mediation of China. Further, two of the arch rivals of the US, China and Russia, are leading members of BRICS, which has become the meeting ground for the friends as well as foes of the US, under the stewardship of China. The US saw all this as a huge challenge to its dominant position in the world and Trump, who was trying to “make America great again”, saw that his dream may go up in smoke. He threatened countries which tried to adopt an alternative to the dollar with sanctions. He may have thought if Iran could be destabilised and structurally broken up, he would be able to kill two birds with one stone. He may have se an enemy of both the US and also its ally Israel and disrupt the BRICS organisation.
The war is affecting the economy of the BRICS countries quite badly. The fuel shortage due to closure of Strait of Hormuz has hit India hard and also China. The economies of the Gulf countries, whose oil is transported via the Persian Gulf and the Gulf of Oman, have also suffered immensely. South Africa, a founding member of BRICS imports oil mainly from the Middle East. Brazil, another founder member, though an exporter of oil, imports refined fuels from the Middle East. A large portion of food requirements also of the Gulf countries come through these sea routes. Thus, the BRICS organisation must be concerned about the consequences of the war if it drags on. It obviously augers ill for the BRICS, and it must act quickly to bring about a ceasefire and an amicable settlement as soon as possible.
Jeffrey Sachs’ opinion
Prof. Jeffrey Sachs, the eminent American economist, has argued that BRICS nations have a critical responsibility to play a leading role in stopping the war in the Middle East, particularly regarding the escalating conflict between the US/Israel and Iran. He contends that because the US is pursuing “global hegemony” and attempting to control the region, BRICS serves as the only effective “standing bulwark” against American domination.
Sachs has stated that if BRICS countries, particularly India, China, and Russia, stand together and demand an end to the war, “it will actually end”. He has described this collective action as the only way to make the world safe. Arguing that the Middle East conflict is a planned campaign by the US and Israel for regional dominance rather than a defensive action, he has called on BRICS to stop the US from running the world. He warned that a continued conflict, especially one that disrupts energy supplies, will cause enormous economic costs for Asia, Europe, and the US.
Sachs has argued that India should not have joined Quad, as he views Washington as using a “divide and conquer” strategy. He has characterised the BRICS countries as a fast-growing, multipolar bulwark that rejects the notion of a single “emperor” (referring to US influence). Sachs has warned that if the conflict is not stopped, it could lead to World War III and catastrophic regional consequences (India Today).
China and Russia, though rivals of the US, have the economic and military clout to exert pressure on the US. India is a friend of both the US and Israel and could act as a mediator to bring about an end to this meaningless war. Gulf countries, some of whom are BRICS members, could make a strong appeal to their friend and benefactor, the US, to see what its senseless aggression is doing to their countries.
Unity of BRICS essential
As of 2026, the expanded BRICS group (including Brazil, Russia, India, China, South Africa, Egypt, Ethiopia, Iran, Saudi Arabia, UAE, and Indonesia) represents approximately 49% of the world’s population. Moreover, its collective GDP is 35 – 40% of the global GDP when measured in PPP terms, which may be considered as higher compared to G7 countries which record 30%. Thus, BRICS is a force to be reckoned with provided its members stand together. However, they have not been able to do so though it is obvious that it would be beneficial to all of them. Bilateral conflicts within the BRICS, apparently intractable, are preventing any concerted action by these countries. In this regard, as Prof. Sachs says the onus is on China, Russia and India to come together to stop the war, which if allowed to drag on, will irreparably damage the economy and unity of BRICS and worse it would never be possible to attain any of its objectives. It is time the founder members Brazil, Russia, India, China and South Africa got together and review its goals, the need for such an organisation as BRICS, and the present danger it faces and take remedial steps as soon as possible if it is to remain a viable force with the potential to counter the hegemonic imperialist forces.
Further, the BRICS, as it consists of stakeholders of a new world order and also countries directly involved in the Middle East turmoil, may have an important role to play in working out an arrangement that could bring permanent and stable peace to the region. Once the dust settles on the military front, and the futility of war becomes apparent it may be time for the BRICS countries to raise a voice to demand a settlement based on the two-state solution that was adopted by the UN. Though Trump brushed this UN resolution aside and started taking over Gaza, once the war is over and he contemplates the economic cost of it to the US public – it costs US 1 – 2 billion dollars a day – he may realize the need for a solution acceptable to all. There have been several US presidents who were strong proponents of the two-state solution—an independent Palestinian state alongside Israel—as a core policy goal. Key proponents included George W. Bush (who first formally backed it in 2002), Bill Clinton, Barack Obama, and Joe Biden; they have viewed it as the most viable path to peace. Israel too after sustaining enormous damage may be forced to agree to a solution, if the US pressures it. Both Trump and Netanyahu, perhaps for personal reasons, wanted a war but they did not expect it to take the turn it has taken. Netanyahu’s days in power may be numbered and Trump may be forced by Republicans to change course as the majority of the US public does not approve of the war.
Therefore, time may be opportune for BRICS to stand together and call for a permanent solution to the Palestinian problem which is at the core of the Middle East conflict. Peace in the Middle East is vital for the further development of BRICS.
by N. A. de S. Amaratunga

Courtesy call by the Heads of Mission- Designate on Prime Minister

Three dead after helicopter crash in Hawaii

Woods charged with driving under influence after crash

Showers may occur at a few places in the Rathnapura, Kaluthara, Galle, and Matara districts during the evening or night

SC finds Keheliya, others, guilty of violating FRs of public through corrupt drug procurement deal

Sajith nudges govt. to follow India’s example in giving relief to consumers by slashing taxes on fuel

‘Dates have the highest sugar content to fight Coronavirus’

Sunday Island 27 December – Headlines

#SundayIsland 17th December – Headlines

Sunday Island – 28th March

Sunday Island Headlines – 21 March

Sunday Island – 21st February – Headlines
-

 News4 days ago
News4 days agoSenior citizens above 70 years to receive March allowances on Thursday (26)
-

 Features6 days ago
Features6 days agoTrincomalee oil tank farm: An engineering marvel
-

 Features13 hours ago
Features13 hours agoA World Order in Crisis: War, Power, and Resistance
-

 News2 days ago
News2 days agoEnergy Minister indicted on corruption charges ahead of no-faith motion against him
-

 News3 days ago
News3 days agoUS dodges question on AKD’s claim SL denied permission for military aircraft to land
-

 Features6 days ago
Features6 days agoThe scientist who was finally heard
-

 Business3 days ago
Business3 days agoDialog Unveils Dialog Play Mini with Netflix and Apple TV
-

 Sports2 days ago
Sports2 days agoSLC to hold EGM in April