Features
COVID-19 Pandemic in Sri Lanka: Contextualizing it geographically – Part I
By Dr. Nalani Hennayake and
Dr. Kumuduni Kumarihamy
Department of Geography, University of Peradeniya
The emergence of a second wave of the COVID-19 pandemic was inevitable, although the sudden outbreak in Minuwangoda took us by surprise. We now see that it is steadily spreading outside of Colombo. The districts of Nuwara-Eliya and, Trincomalee have been declared as areas not suitable for tourist activities, and pilgrimage to Sri Pada is discouraged. Kandy, where we live is the fourth district in terms of the total number of COVID-19 positive cases detected. The actual reality of the COVID-19 pandemic, changing nature of the virus, how many are infected, detected, tested, and identified as infectious, where they live, work, and move around, could be far beyond what statistics and dashboards may reveal.
Along with the health and security personnel, the government successfully managed the first wave with a series of controlling strategies from travel restrictions, imposed quarantines, self, and institutional isolations. Interestingly, all such strategies, have been territorial or spatial measures. In other words, the management of the COVID-19 pandemic requires a set of spatial strategies that affect human spatial behaviour, relations, and attitudes. Inspired by this, in this article, we 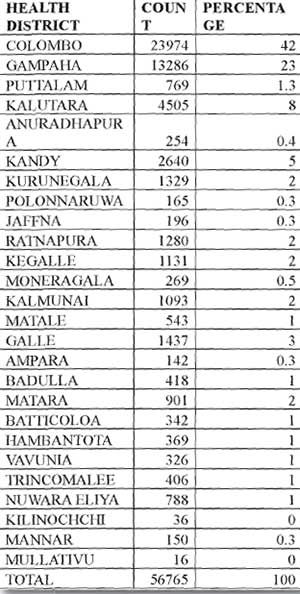 embark upon a project of contextualizing the COVID-19 pandemic in Sri Lanka, geographically. This article aims to show the significance of a geographical framework of thinking, with limited data and information. In other words, what we present here is a sample of what can be done if the data are available at the GN division level. Such an analysis would demonstrate how geography is an innately central character of how COVID-19 is spread, dealt with, and, most importantly, in an academic perspective, in representing, analyzing, and understanding the present situation and future scenarios of the pandemic.
embark upon a project of contextualizing the COVID-19 pandemic in Sri Lanka, geographically. This article aims to show the significance of a geographical framework of thinking, with limited data and information. In other words, what we present here is a sample of what can be done if the data are available at the GN division level. Such an analysis would demonstrate how geography is an innately central character of how COVID-19 is spread, dealt with, and, most importantly, in an academic perspective, in representing, analyzing, and understanding the present situation and future scenarios of the pandemic.
Current situation: What is reported, recorded, and represented?
In its Situation Report on February 3, 2021, the Epidemiology Unit at the Ministry of Health reports 65,698 as ‘the total number confirmed’ and 59,883 as ‘the total number recovered’ COVID-19 cases. Thus, we have only 5485 patients as confirmed and hospitalized, with 548 added as suspected and hospitalized patients. The other basic information provided on this website is the district-wise and hospital-wise distribution of the total number of confirmed patients. The highest number of COVID-19 patients, nearly about 42 percent, comes from the Colombo district, while Gampaha and Kalutara record respectively about 23 and 8 percent (see Table 01) Nuwara-Eliya-Ratnapura. The number of COVID-19 infected seems to increase in the districts of Kandy, Kurunegala, Puttalam, Nuwaraeliya, Rathnapura, Kegalle, Galle, Badulla, and Kalmunai.
Table 01: District Distribution of Confirmed Patients (as of February 3, 2021 -10 a.m, Situation Report)
Note:
Considered only the individuals who contracted the disease from the districts
How the COVID-19 pandemic is reported and represented in the media and various sources is all the more confusing. The statistics coupled with the newscasters’ tone (depending on which channel you watch the news in the evening) determine the outbreak’s nature for the day. Frequently, in the middle of the regular news reporting, we hear, “Here we received some new information right now” – new COVID-19 cases added – leaving us with a sense of uncertainty as to how this coronavirus proliferate daily. Generally, during the first wave, the media played a crucial role in raising awareness about the COVID-19 pandemic and sensitizing the people towards the situation with their frequent announcements and reminders. Such an effort is not noticeable during the second wave. Perhaps, the ‘new normal’ has become normal. The new cases are generally attributed to the four clusters. As of February, 2021, the Minuwangoda cluster has proliferated up to 61,705 cases, as it is reported on the relevant official websites. At different phases of the second wave, Peliyagoda and Prison clusters were also added to the Minuwangoda cluster. In the popular memory, informed by the official line and the format of reporting by various channels and mainstream media, such reporting creates an impression that it is still the Minuwangoda/Peliyagoda cluster that is expanding as if it has not yet spread to other parts of the country.
The first wave of the outbreak that began with the case of the Chinese tourist and lasted until almost late April 2020 was well controlled before the general election, through strategies such as physical distancing, quarantine, contact tracing (social, temporal, and spatial), lockdown, and isolation of villages and communities and travel restrictions. The first wave witnessed that restricting and controlling human spatial conduct and mobility are the determinants of preventing further transmission of the coronavirus. The government took strict measures to control human spatial mobilities through curfew and prolonged lockdowns at the provincial and, at times, even at the national level. It is reasonable to say that controlling human spatial mobilities has been a successful strategy in curtailing the first wave, enhanced by the commitment and dedication of the health, security, and various other sectors. However, during this first wave, the coronavirus carriers were identified as foreigners of two kinds instead of locals. They are the immigrant workers who had returned from the Middle East and Italy and a small number of actual foreigners visiting Sri Lanka. The exception to this was the Welisara Navy outbreak and small groups of the infected in a few low-income localities in Colombo. Thus, the coronavirus had not fortunately been ‘socialized’ into the local society.
At present, the second wave that began in early October, when an employee from a garment factory in Minuwangoda was found positive for COVID-19, is different. Although it was debated in the early days whether the coronavirus had still come through ‘foreigners,’ it is clear that the virus is, by now, ‘indigenous‘ to us. It took a while to acknowledge that the coronavirus is ‘socialized‘ – meaning that it is out there with us. It is imperative to know the geographical spread of the COVID-19. This is important for the decision-makers to enact necessary controlling mechanisms (i.e., isolation, lockdown, inter-regional restrictions on mobility, etc.) in the relevant regions, places, and localities on the one hand, and on the other, for the individual citizens to safeguard themselves from the coronavirus and to prevent its further transmission. Looking at the COVID-19 pandemic geographically is far beyond a simple exercise of mapping where the COVID-19 cases are found and located. The COVID-19 pandemic has changed the geography of the world. Under pre-pandemic normalcy, spatial and geographic barriers are removed within the capitalist system to facilitate a smooth expansion and circulation of capital and commodity markets. The resultant flat geographical surface is what made the globalization of the COVID-19 pandemic possible. However, the COVID-19 pandemic has reversed this as the countries resort to spatial and geographical restrictions (lockdown areas, restricted mobilities, isolated villages, high- risk, low-risk areas, etc.) to control the pandemic. Thus, we must contextualize and unravel the geographical dynamics of the COVID-19 pandemic to gauge its extent, scope, and severity and reevaluate the efficacy of the controlling strategies and problematize it further.
Geographical contextualizing of the pandemic
Contextualizing the COVID-19 pandemic in Sri Lanka would involve a range of geographical inquiries, analysis, and interpretation that spans from a simple mapping exercise to analyses of socio-cultural, economic, and political dynamics of the communities/ localities where the infected are detected. Geographers’ holistic and integrative perspective allows any phenomenon to be viewed in an interdisciplinary manner and a synthesized form. A geographical line of inquiry, on the one hand, enables the decision-makers to foresee and plan for the future scenarios in terms of, especially, risk areas (for containing the COVID-19 as well recovering the economy) and also to implement the controlling strategies more efficaciously and in a socially more responsible manner. On the other hand, such an exercise helps the public to understand the extent, scope, and severity of the crisis and to reflect individually upon the ethics of personal conduct necessary to prevent the further social proliferation of the coronavirus. Here we use the three themes of infection, vulnerability, and immunization to focus on COVID-19 in Sri Lanka geographically; out of seven themes (infection, vulnerability, resilience, blame, immunization, interdependence, and care) introduced in the Editorial, the Transactions of the Institute of British Geographers (volume 45 of 2020). In addition, we introduce ‘social distancing’ as a form of micro-geography of COVID-19 since it enfolds a set of human spatial interactions involving spatial distancing at the individual level.
Geographies of infection
: With the first wave, particular places, except for Atalugama and a few low-income localities in Colombo were not identified with COVID-19. A majority of the infected were detected from those retained at the quarantine centres. Now, with the second wave, it is different. The questions of where the infected have been found, where they live, where they have been, and what kind of neighborhoods they have been found from are critical information relating to the transmission and control of COVID-19. At the global level, universities, research institutes, and various geo-visualization sites have produced maps demonstrating the global nature of COVID-19. They are mapped not only at the national scale but also covering the regional and local scales. In these global maps, Sri Lanka was earlier highlighted as a country that managed to control the COVID-19 successfully in the first wave with an insignificant number of fatalities. With the second wave, we are now reported as “at peak and rising at a rate of 16 infected per 100K people during ‘the last seven days’ (See the REUTERS COVID-19 TRACKER). Sri Lanka is classified as a country at 75% of the peak of the infection curve with a daily average of 523 new infections. In these global analyses, Sri Lanka places itself at the lowest end, compared globally and within Asia and the Middle East, regarding the total infections, deaths, average daily reported, and total per population. The relatively low position of the country’s outbreak in its region and the world should not be used, especially by the politicians, to downplay its severity at the national level. It is interesting to note that most of the news channels, immediately after reporting the outbreak’s national situation, instantly turn to the pandemic’s global standing, highlighting its severity, almost making the Sri Lankan situation, so to say, uneventful and insignificant. The politicians often tend to overemphasize this as a GLOBAL pandemic to escape from criticisms and lessen its significance at the national level.
(To be continued)

The S.J.V. Chelvanayakam KC Memorial Lecture delivered on 26 April, at Jaffna Central College, by Professor G.L. Peiris, an academic with outstanding credentials, was published, under the title, “Federalism and paths to constitutional reform,” in The Island of 27 April, 2026.
In Part II of the publication, titled “Advocacy of Federalism: Origins and Context,” Professor Peiris states: “At the core of political convictions he held sacrosanct was his unremitting commitment to federalism…”. Contrary to popular belief, however, federalism in our country had its origins in issues which were not connected with ethnicity. At the inception, this had to do with aspirations, not of the Tamils but of the Kandyan Sinhalese. The Kandyan National Assembly, in its representations to the Donoughmore Commission in 1927, declared: “Ours is not a communal claim or a claim for the aggrandizement of a few. It is the claim of a nation to live its own life and realise its own destiny”.
Commenting on S.W.R.D. Bandaranaike’s views, Professor Peiris states: “Soon after his return from Oxford, as a prominent member of the Ceylon National Congress, was an advocate of federalism. He went so far as to characterise federalism as ‘the only solution to our political problems”.
THE COMMON THREAD
The thread that is common to the sources cited above is that while their focus was on the political framework, there is not even a hint as to the territorial units to which the political framework of federalism is to apply. With time the Tamil “nation” claimed that their federal State was to be the Northern and Eastern Provinces of Sri Lanka. However, the Kandyan “nation” was silent on this issue. Since Britain annexed the Kandyan Kingdom and the unified, then Ceylon in 1815, for all intents and purposes it would be reasonable to assume that the claim of the Kandyan “nation” was to be the region under the last Kandyan King, leaving the Western and Southern coastal regions for the Rest of the “nation”.

Chelvanayakam
Sri Lanka, while being a colony under the British, was not interested in political frameworks. Instead, the British were interested in structural arrangements that facilitated Administration. It is evident from the evolutionary processes explored by the British that subdivided units of a State are critical not only for effective Administration but also for the political framework that ensures political stability. Federalism, advocated by the Tamil and Kandyan Leaderships for territorial units, as claimed by them, would inevitably lead to political instability. The lesson to be learnt is not to start with political frameworks, such as Federalism, but to first decide on the territorial units, within which a State functions, to ensure stability, and then frame political aspirations of the People belonging to such a State, in order to ensure political and structural stability.
LESSONS of HISTORY
Material from an article, dated 16 June, 2016
“When the British took control of the Dutch possessions in former Sri Lanka, in 1796, the Kandyan Kingdom was independent and separate from the Maritime region. The Kandyan Kingdom consisted of the “central highlands with the eastern and southeastern coastal strips”. It was after ceding of the Kingdom, at the Kandyan Convention of 1815, and after the rebellion of 1817-1818, that the two regions were merged. However, despite the merger, the administration of the two regions remained divorced from each other, with the Kandyan region being divided into 11 Districts, and the Maritime region into five, creating a total of 16 Districts for the administration of the whole country (Sir Charles Collins, Public Administration of Ceylon, 1951, p. 49).
“The above arrangements continued until the recommendations of the Colebrook – Cameron Commission. In 1832, the recommendations of the Commission were accepted , “… and the separate administrative system for the Kandyan provinces was abolished and amalgamated with the territories on the littoral acquired from the V.O.C. in a single unified administration structure for the whole island. The existing provincial boundaries within the two administrative divisions – the Kandyan and maritime provinces – were redrawn, and a new set of five provincial units, of which only one – the Central Province – was Kandyan pure and simple, was established. The new provincial boundaries cut across the traditional divisions and placed many Kandyan regions under the administrative control of the old maritime provinces” (K.M.de Silva, A History of Sri Lanka, 1981, p. 263), continued until as late as 1889, resulting in nine Provinces for the sole purpose of facilitating the Colonial administration. In point of fact, the Province never functioned as the administrative unit. Instead, the administrative unit was essentially the District, and the situation has remained so throughout the Colonial period and into this day. According to Sir Charles Collins cited above: “Most provinces were divided into districts, each Government Agent having charge of his own district, with general supervision over the whole province. The districts not in the direct charge of Government Agents were under the control of assistant Government Agents”. (Ibid, p. 62.)
PRIORITISING POLITICS OVER STABILITY
The lesson learnt by the British was that if a Colony is to be Administered effectively, the Colonizer had to choose the most appropriate unit of administration. Similarly, to an Independent Sovereign State, Territorial Stability should be its foremost priority. This means deciding on the most structurally secure territorial unit within which political power sharing should operate and not prioritise political frameworks, such as Federalism, at the expense of the structural stability of the State. Political instability would have been inevitable had Sri Lanka succumbed to pressures from the Tamil and Kandyan Leaderships.
Although Britain was not concerned with territorial stability, they recognised that the District was the most effective unit for effective administration. In fact, the 1977 Constitution describes the Territory of Sri Lanka in terms of Administrative Districts. Despite this, it was the Indo-Lanka Accord that first recognised the Northern and Eastern Provinces as political units. Following this, the 13th Amendment of 1987 extended this recognition to all Provinces.
The adoption of the Province as the political unit may not have had an impact on the territorial integrity of the Sri Lanka State, except for the Northern and Eastern Provinces, judging from the events that followed over three-plus brutal decades. The transformation of the territory of Sri Lanka, from Administrative Districts to Provinces and Provincial Councils, is the direct result of prioritising politics over territorial stability. For India to be the handmaiden of this transformation is beyond comprehension because instability in Sri Lanka, in whatever form, would impact on India’s own territorial integrity. This serious blunder cannot be ignored any further for the sake of both Sri Lanka and India. It is imperative that measures are taken to engage in a course correction through Constitutional Reform.
PROPOSED CONSTITUTIONAL REFORMS
The path to Constitutional Reform should start with the territorial subdivision of the Sri Lankan State into Districts, not only to ensure the territorial integrity of the State but also to improve administrative and development efficiencies coupled with Local Government units; a lesson learnt from the British. Any political powers devolved/decentralised to Districts should be the responsibility of District Councils, elected by representatives to Local Governments within each District.
Political power at the Centre should reflect the commitment to a single Sri Lankan Nation, through an elected Legislature, with Executive Powers being shared by a President/Prime Minister, with a Cabinet made up of all communities, in the ratio represented in Parliament. An attempt to share Executive Power with all communities, in an inclusive Cabinet, has not been the practice in the past, and under the present government, as well, despite its strident calls for unity and reconciliation. Consequently, the tendency for minority communities is to seek peripheral power to the maximum extent possible.
CONCLUSION
The approach to Constitutional making has been how best to accommodate political power in the form of Federalism, first by the Kandyan “nation” and later by the Tamil “nation”. The claim by the Tamil Leadership morphed from Federalism to a Separate State resulting in tragedies of an unimaginable order, to the point of threatening the very existence of the Sri Lankan State.
The current arrangement is based on Power being devolved to Provinces, in the form of Provincial Councils, with no regard the Province, makes to the territorial durability of the Sri Lanka State. How successive Governments hope to prevent threats to territorial vulnerabilities is to curtail the operation of sensitive provisions of devolved powers. This is being disingenuous.
On the other hand, the more direct and forthright approach to Constitutional Reform is to make the District the unit of peripheral power in order to ensure territorial stability and effective peripheral development and share Executive Power with communities in the ratio of their representation in the Legislature. The first could be achieved through a referendum and the second by the President/Prime Minister of any government. This approach prioritises territorial stability over political power; a change that has eluded policymakers. Therefore, it is imperative that territorial stability is given the foremost place in Constitutional Reform processes for the sake of not only Sri Lanka but also for India, for reasons of connectivity.
by Neville Ladduwahetty

The power cuts are already here. Perhaps, even before the date predicted by the Public Utilities Commision of Sri Lanka (PUCSL. The peak load has gone well past the threshold they indicated as the tipping point of 3030 MW of peak load. It is now will past 3100 MW and growing, perhaps triggered by the continued heatwave making the use of air conditioners and fans more frequent and by a wider group of consumers. The government insists there is no intention of power cuts but each of us have experienced some form of power outage, without notice, at some time or other.
It is in this scenario that the Ceylon Electricty Board (CEB), or whatever it is called now, had directed all roof top solar projects, over 300 MW capacity, to shut down for the period 10th April to 20th April.
This is in addition to the curtailment of all ground mounted solar and wind projects, and even mini hydro projects, without compensation, going on for some months.
One year of inaction by CEB with the problem staring in the face
If will be recalled that the same demand was made in April, 2025, after the debacle of the countrywide blackout on 9th February, 2025, whether caused by a monkey or otherwise.
The question to be raised is what steps have been taken by the then CEB, or the Ministry to anticipate the situation this year, too, and to try and mitigate the same.
The easy answer is absolutely nothing. If at all what has been done is unilaterally prevent any further addition of Roof Top Solar PV, under the provisions of the Surya Bala Sangramaya (SBS), is, undoubtedly, the only short term and economical means to add low cost renewable electrical energy to the grid.
The architect of the SBS, the Sustainable Energy Authority is deafening by their silence, when their signature project of prime national importance has been sabotaged, and now even the performance of the already installed systems are being curtailed.
This action is totally unbelievable when the use of expensive oil-based generation will continue unabated, even during the day, when there is so much solar energy already installed. Of course, the age-old excuse will be trotted out, of the non-firm nature of Solar and Wind and problems of grid stability, etc.
Many useful and practical solutions to face the growing issue of how to integrate the essential low cost but variable resources of solar and wind to the grid as an aftermath of the blackout were discussed over a year ago.
But nothing seems to have even been attempted. The most prominent among these was the proposal to add 300 MW of grid scale batteries, as indicated in the already-approved Long Term Electricity Generation Plan ( LTEGP 2024 – 2044,) of which 100 MW should have been in use by 2026. The tender for the addition of 16 X 10 MW battery storage at selected grid substations was called over a year ago. Some expectation of sanity
It is under these circumstances that the PUCSL called for a stakeholder consultation on the 10th April, 2026, after circulating a concept note, which was well attended. It was a breath of fresh air, in view of the downhill slide of the entire electricity sector in the recent months compounded by the raging controversy of the coal scam and the rapidly increased use of expensive diesel, in addition to the other fossil fuels, just to keep up the generation to match the demand. The double whammy of the doubling of the fuel prices , exacerbated the hit on not only the consumer’s monthly bill, but the national economy and balance of payments.
Therefore, it was most encouraging to note from the PUCSL’s concept note that sanity has prevailed at last. We have been demandin–g some concrete strategies and time based targets to rid at least the electricity sector from the use of expensive, polluting fossil fuels, commencing with oil. This is the only means by which the utility could hope to achieve some degree of economic and financial viability. They have continued to burden the consumer and the country by continually jacking up the consumer tariff, while ignoring any prudent means to clean up their Act. As a matter of interest, the CEB’s own data of 2023 shows that it is possible to save some Rs 113 Billion annually by replacing all oil-based generation using renewables. The country could have saved over $ 700 Million in Foreign Exchange and the Consumer Tariff could have been lowered by Rs 7.00 per Unit across all segments of consumers.
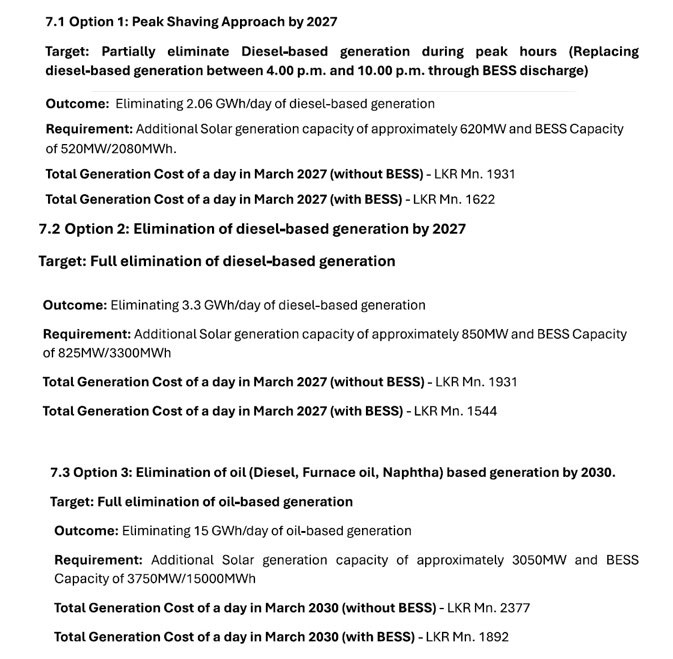
Therefore, the PUCSL concept paper out lines, some credible measures to eliminate the use of all of forms of oil for power generation in stages. The three tier of approach, outlined as option 1 to 3, reproduced here, should be commended for adopting a pragmatic approach, with very good chance of success.
Proposed options by PUCSL
(See Options 1 Peak Shaving Approach by 2027 and Option 2: Eliminating 2.06 GWh/day of diesel-based generation)
Considering even the recent past when we achieved a status of zero oil use, as compared to the present sorry status, this is not an extremely difficult task. We will have to substitute Solar PV to bridge the gap of reduced Hydro during dry months.
(See diagram 1)
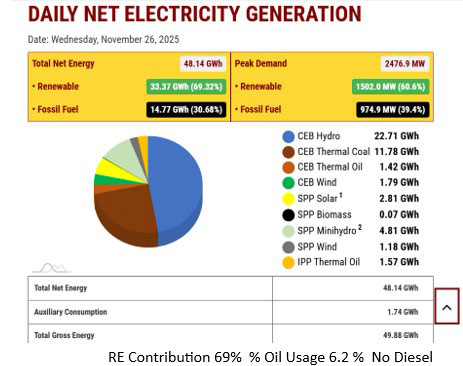
RE Contribution 69% % Oil Usage 6.2 % No Diesel
(See diagram 2)
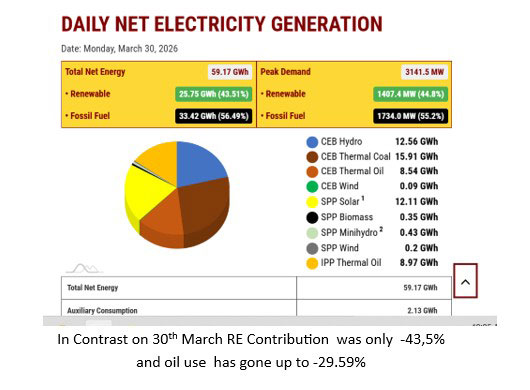
In Contrast on 30th March RE Contribution was only -43,5%
and oil use has gone up to -29.59%
However, as outlined in the introductory paragraphs of the concept paper, the driving force to promote this change is the early declaration of appropriately worked out tariffs for installation of storage batteries and delivery of the stored energy to the grid.
With the total lack of progress of proposals in the LTEGP 2025-2044 by the state institutions, it is prudent to assume any future initiatives can only come from private sector participation.
Using the power granted by the recently ratified Electricity Act NO, 36 (As amended) the PUCSL has moved with commendable speed to develop the Feed in Tariff declarations needed to enable the achievement of the above objectives and a further stakeholder consultation was held on the 24th of April when more detailed proposals were put forward.
However, although the responsibility of publishing the tariff remains with the PUCSL, unless the National System Operator ( NSO ), tasked with the planning and implementation of Electricity Sector developments , takes urgent action to implement the desired changes as a highest priority task, nothing will be gained to help the country to get out of this quagmire.
The Consumer Continues to be Burdened.
Further, as the time table proposed by the PUCSL itself indicates, even the first of the options can be implemented only in 2027, with the others following up to the year 2030.
These are very encouraging time targets and the consumers will eagerly await their achievement.
However, the threat of power cuts, as well as continuing increase in consumer tariff to fuel the use of diesel for power generation, is real and current. A further tariff increase of 18% has been demanded by the NSO, on top of the 15% granted on 1st April, 2026.
The Immediate Options Available to Consumers.
a) The CEB now refuses to provide any grid connection for integration of any rooftop solar PV systems under the Surya Bala Sangraamaya.
b) The only way available to the consumers is to install Off grid roof top solar systems with adequate batteries to be none dependent on the grid. Use the grid only during the off peak hours.
c) During most periods of the year, even under cloudy conditions there is some solar generation. To ensure the daily consumption is more than covered by the solar input and any surplus is used to charge the battery, to the level adequate to manage the evening and peak hour demand, the capacity of the solar panels and battery have to be determined.
d) It is to be noted that although only the relatively high-end domestic consumers could find the proposed scheme financially feasible under the present cost regimes, which will improve further when the second tariff increase is announced shortly, to those consuming over 250 Units/Month, their engagement has a sector wise positive implication which is beneficial to all levels of consumers.
e) The scheme will operate in an off grid mode, without exports to the grid at any time. Therefore, they will not contribute to the often voiced worries of over voltage, instability and variability in the national grid.
f) Once the PUCSL announces the required FIT and the NSO or the Distribution Companies institutes the necessary facilities, such as smart meters, such consumers, too, can further assist the grid by export of any excess they generate.
Proposal to Avoid Power Cuts Implementable by Domestic Consumers
There are several drivers which will attract the potential ” Prosumers” to adopt this option without delay.
* The consumer tariff will continue to rise
* Even the former Roof Top Solar Systems, without batteries, does not provide power during the power cuts or blackouts
* At present day prices, the investment is financially feasible, based on the savings of the current level of monthly electricity bill. A substantial bank loan can be comfortably settled from the savings
* Now cooking with electricity is no longer a financial burden but can save one from the cost and danger of LPG shortages and queues
* What you, do based on your economic ability, will be a service to all consumers as the resultant reduction of Peak Demand means the use of Diesel can be gradually reduced and the lower end consumers, too, will benefit.
* You will enhance your green credentials with your own financial benefits.
The overall benefit to the grid and other consumers
If the element of exorbitant cost of diesel-based generation is removed then there is no need for the increase of consumer tariff for all consumers.
What is more important is that trimming the peak load would drastically reduce the need for any power shredding that is happening on the sly now and thereby benefit all consumers,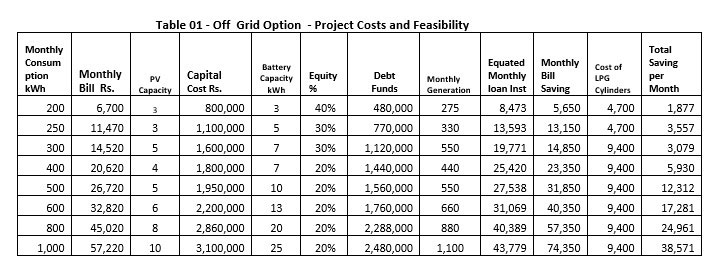
The summary of Financial Analysis illustrating the viability based on currently available data is given here. This will improve drastically if a further increase in consumer tariff is granted, which appears inevitable. (See Table 01 – The basic data used for this analysis is available on request.)
by Eng Parakrama Jayasinghe
parajayasinghe@gmail.com

In a striking symbol of the global energy transition, vast stretches of once-abandoned coal mines in China have been reborn, not as relics of an industrial past, but as shimmering hubs of renewable energy.
What were once scarred landscapes, destabilised by years of mining, and later submerged by landslides and floods, have now been transformed into expansive artificial lakes.
Floating atop these waters are some of the world’s largest solar power installations, quietly generating clean electricity on a massive scale.
Among the most notable are the Fuyang Floating Solar Farm and the Huainan Floating Solar Farm. Together, they represent a remarkable engineering and environmental achievement.
The Fuyang facility boasts an installed capacity of 650 megawatts, producing approximately 700 million kilowatt-hours of electricity annually. Even more impressive, the Huainan project reaches a staggering 1 gigawatt capacity, generating nearly 1.8 billion kilowatt-hours each year. Combined, these floating giants produce enough electricity to power millions of homes without burning a single lump of coal.
A former General Manager of the Ceylon Electricity Board (CEB), a veteran electrical engineer, described the development as “a glimpse into the future of energy systems.”
“What China has demonstrated is not just technological capability, but strategic foresight. Turning environmentally degraded land into clean energy assets is the kind of thinking countries like Sri Lanka must begin to adopt,” he said.
Why solar on water?
Floating solar, or “floatovoltaics,” offers a range of advantages that traditional land-based solar farms cannot easily match.
Water naturally cools solar panels, improving their efficiency by an estimated 10 to 15 percent. In hot climates, this cooling effect can significantly boost electricity generation.
Additionally, the panels reduce water evaporation, a crucial benefit in regions facing water stress. By limiting sunlight penetration, they also help suppress algae growth, improving water quality.
Perhaps, most importantly, floating solar eliminates the need for large tracts of land. In densely populated or agriculture-dependent countries, this is a game changer.
A dual economy: Fish and power
In an innovative twist, some of these floating solar farms incorporate aquaculture beneath the panels. Known as the “fisheries + solar” model, it allows communities to cultivate fish in the shaded waters below, creating a dual-income system, energy production above, food production below.
This integrated approach not only maximises resource use but also supports local livelihoods, blending sustainability with economic resilience.
Environmental dividends
The environmental benefits are substantial. The Fuyang project alone reduces carbon dioxide emissions by an estimated 580,000 tons annually, while the Huainan facility cuts emissions by around 1.6 million tons each year.
Beyond emissions, these projects reclaim landscapes once deemed unusable—areas heavily damaged by coal extraction. In doing so, they rewrite the narrative of industrial decline into one of ecological restoration and innovation.
Sri Lanka: A nation poised for floating solar For Sri Lanka, the implications are profound.
Unlike China’s abandoned coal pits, Sri Lanka possesses thousands of irrigation tanks, reservoirs, and hydropower catchments that could serve as ideal platforms for floating solar. From the ancient tank systems of the dry zone to major reservoirs like Victoria Dam and Randenigala Reservoir, the country holds untapped potential to generate clean electricity without sacrificing precious land.
The country’s reliance on thermal power, particularly during drought periods when hydropower declines—has long been a challenge. Floating solar could provide a stabilising solution, reducing dependence on costly fossil fuels while complementing existing hydroelectric infrastructure.
Energy analysts note that integrating floating solar with hydropower reservoirs can create a hybrid system: solar power during the day, hydropower balancing supply at night. This synergy enhances grid stability and reduces overall generation costs.
The former CEB official stressed the urgency:
“Sri Lanka cannot afford to delay. With rising energy demand and climate pressures, we must explore every viable renewable option. Floating solar on our reservoirs is one of the most practical and scalable solutions available.”
Challenges and the road ahead
However, experts caution that careful planning is essential. Environmental assessments, grid integration, and financing mechanisms must be properly addressed. Community engagement, especially where fisheries are involved—will also be key.
Yet the blueprint already exists.
China’s transformation of submerged coal mines into renewable energy hubs offers more than inspiration—it provides a working model. For Sri Lanka, adapting that model to its own geography could mark a decisive step toward energy independence.
China’s floating solar farms stand today as one of the clearest symbols of a world in transition—from fossil fuels to renewables, from environmental degradation to restoration.
For Sri Lanka, the message is equally clear: the future of energy may not lie on land alone—but on water, where sunlight meets innovation.
If harnessed wisely, Sri Lanka’s vast network of reservoirs could one day mirror that transformation, turning calm waters into engines of sustainable growth.
by Ifham Nizam

Maldivian President plants a sapling to mark 60 years of Sri Lanka–Maldives Diplomatic Relations

Sri Lanka and Maldives strengthen ties with productive bilateral talks

Maldives and Sri Lanka exchange seven MOUs

Warm Welcome Accorded to the President of the Maldives at the Presidential Secretariat

Modi’s BJP conquers Bengal, one of India’s toughest political frontiers

PM participated in ’Swarnabhivandana 2026,’ Sacred Relic Veneration Ceremony

‘Dates have the highest sugar content to fight Coronavirus’

Sunday Island 27 December – Headlines

#SundayIsland 17th December – Headlines

Sunday Island – 28th March

Sunday Island Headlines – 21 March

Sunday Island – 21st February – Headlines
-

 News6 days ago
News6 days agoTreasury chief’s citizenship details sought from Australia
-

 News5 days ago
News5 days agoRooftop Solar at Crossroads as Sri Lanka Shifts to Distributed Energy Future
-

 News4 days ago
News4 days ago“Three-in-one blood pressure pill can significantly reduce risk of recurrent strokes”
-

 News7 days ago
News7 days agoGovt. assures UN of readiness to introduce ‘vetting process’ for troops on overseas missions
-

 Business7 days ago
Business7 days agoADB-backed grid upgrade tender signals next phase of Sri Lanka’s energy transition
-

 News6 days ago
News6 days agoCentral Province one before last in AL results
-

 Sports6 days ago
Sports6 days agoWell done AKD!
-

 Business7 days ago
Business7 days agoUpdate on independent forensic review