Life style
When it was known as the Harley Street of Ceylon
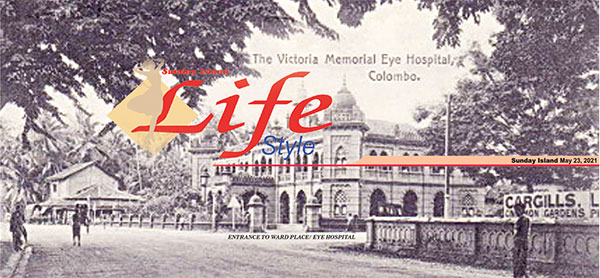
The Homes in Ward Place in its early days,
by Hugh Karunanayake, Dr Srilal Fernando, and Avinder Paul
Ward Place in the heart of Cinnamon Gardens is a roadway linking the epi centre of the Colombo Municipality with the eastern area of metropolitan Colombo. Two centuries ago, there was no roadway in the area, which was part of cinnamon plantations established during the Dutch period of occupation of the maritime areas of Ceylon. When a road to the area was first built in the nineteenth century it was named Borella Road, later to be named Ward Place.
Arunachalam Ponnambalam was a man of foresight and great acumen. Originating from the village of Manipay in the north of the island, he sought opportunities for work in Colombo during early British times and won the confidence of British Governors who appointed him the Chief cashier of the Colombo Kachcheri which was the key government instrument in the administration of the dominion of Ceylon. The Kachcheri together with the early Legislative Councils were the local institutions that set the pace for the administration of the colony. Land throughout the country was made available by the new rulers of the island at ome to five shillings per acre to pioneer British settlers, and also to a few natives who had won the favour of the Government.
 Arunachalam Ponnambalam was one of the latter, and by the mid 1850s the owner of two cinnamon estates, Rajagiriya, and Borella. While Rajagiriya Estate was sold after some years, to Mrs Cornelia Obeyesekera whose son Donald established a township still known as Obeyesekera Town, Borella Estate disintegrated into building blocks for residential housing. Ward Place of today represents a part of the original Borella Estate.
Arunachalam Ponnambalam was one of the latter, and by the mid 1850s the owner of two cinnamon estates, Rajagiriya, and Borella. While Rajagiriya Estate was sold after some years, to Mrs Cornelia Obeyesekera whose son Donald established a township still known as Obeyesekera Town, Borella Estate disintegrated into building blocks for residential housing. Ward Place of today represents a part of the original Borella Estate.
Ward Place, named after British Governor Sir Henry Ward, became an elite residential area not long after the Ceylon Medical College was established in the adjoining Regent Street in 1870 with Dr Edwin Lawson Koch as its first Principal. This was followed two decades later by the Victoria Memorial Eye Hospital built through the munificence of the legendary 19 Century philanthropist Sir Charles Henry de Soysa. Another landmark event in the progress towards enhanced healthcare was the establishment of the De Soysa Lying-in-Home (the LIH) on December 13th, 1879. The hospital owes its beginning to a philanthropic gesture by Sir Charles Henry de Soysa.. He was deeply touched by the plight of women of poor socio-economic status who were deprived of the facility for safe care in a hospital during childbirth. He proceeded to establish a hospital by personal donation of property and funds for their care, the De Soysa Lying-in-Home which is the second oldest maternity home in Asia.
Since then it has played the lead role in providing for all aspects of healthcare for women and in the training of staff in all grades for this field of work. During the initial years, maternity services was the main thrust of activities at De Soysa Lying-in-Home. At its commencement it consisted of 22 beds and provided for 52 births during its first year. A decade later the hospital was providing for 425 births annually then on to 1051 in 1909 and 2000 in 1921. The bed strength had now increased to 100. In later years it provided care for over 14,000 maternity cases annually, most of which are of a high-risk nature. Today it is a Teaching Hospital.
The Victoria Memorial Eye Hospital stands on a property formerly named Mango Lodge which was said to have been a hunting cabin during the time of the Dutch occupation. The two institutions viz the General Hospital and the Eye Hospital served as the pioneer medical institutions of the country, and attracted most of the country’s medical specialists for service there. Consequently, Ward Place became the most sought after location for residence for medical specialists and by the beginning of the 20th Century was the most popular residential location for leading medical specialists., and regarded as the Harley Street of Colombo.
The General Hospital (as it was then known) was established during Sir Henry Ward’s governorship (1855-1860), with 3,000 pounds sterling being earmarked for the project. Until then, government policy had been to contribute to locally operated charitable health organisations. However, after the establishment of the General Hospital, this policy was abandoned. Furthermore, the General Hospital also succeeded the Pettah Hospital, since the latter’s capacity to treat patients was very low.
Accordingly, the General Hospital was opened in Longden Place in 1864, under the inaugural administration of Civil Medical Officer Dr Parsley .It was later moved to Kynsey Road. named after its first Medical Superintendent, Dr WR Kynsey. The location of the General Hospital added to the demand for specialist medical services, which in turn created a soaring demand for residential accommodation to which Ward Place was considered the prime locale.
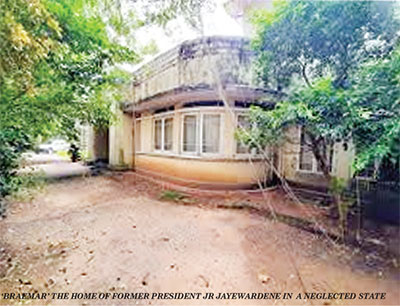
Perhaps the best known resident of Ward Place was Former President JR Jayewardene, who lived in a house named “Braemar” at 66, Ward Place. The property was originally owned by his father-in-law, Leonard Rupesinghe whose only child, Elina, was married to JR. It is on record that he bought the property from a previous owner, most probably a Scotsman, who had bestowed the name Braemar on it. C Brooke Elliott the lawyer lived there as a tenant, when he published his book “Real Ceylon ” in 1938. Since then the original house had been demolished by Rupesinghe, and by the Jayewardenes who built a modern residence for themselves, retaining the old name Braemar. The house has since been ascribed to the Inland Revenue Department to offset income taxes, but is being managed by the JR Jayewardene Cultural Centre.
 Another famous resident of Ward Place was Sir Ponnambalam Ramanathan, the national leader of the early Twentieth Century. His stately home named Sukasthan was demolished several decades ago to give way to the construction of many large homes on the property which now have the address Sukasthan Gardens. It could be speculated that Sir Ponnambalam built his home on land inherited from his father Arunachalam Ponnambalam from the Borella Estate.
Another famous resident of Ward Place was Sir Ponnambalam Ramanathan, the national leader of the early Twentieth Century. His stately home named Sukasthan was demolished several decades ago to give way to the construction of many large homes on the property which now have the address Sukasthan Gardens. It could be speculated that Sir Ponnambalam built his home on land inherited from his father Arunachalam Ponnambalam from the Borella Estate.
The list of names of residents of Ward Place in the early 20th century would read as a list of the most eminent personae of the medical profession in Ceylon of the time. Names such as Dr Simon de Melho Aserappah, his son-in-law, Dr SC Paul, the latter’s son Dr Milroy Paul, possibly the only holder of the Master of Surgery qualification from Ceylon. There was the reputed eye surgeon Sir Arthur M de Silva, gynaecologist Dr PR Thiagarajah, Dr Percy Kulasinghe, Dr SL Navaratnam, Dr Jackie de Silva, Dr DP Billimoria, Dr W Balendra, Dr AC Arulpragasam, Dr A Sinnatamby, and Dr LAP Britto Babapulle are names that readily come to mind, and were household names of mid Twentieth Century Ceylon. There would of course be many others.
The residents of Ward Place were the elite of Colombo’s society and the medical practitioners living there commanded the biggest practices and were considered as the crème de la crème of medical specialists in the country, with a few exceptions of course.
At the intersection of Ward Place with Alexandra Place stood the two storied home of Dr Alles on a 120 perch block of land. It was for many years subsequently leased by the government of the day as the head office of the Department for the Registration of Motor Vehicles. The Alles property was next to the original home of Cargills Pharmacy which later moved to the opposite end of the De Soysa Circus .For the past few decades It was operating as a retail fashion centre named ODEL , a concept new to the country and successfully owned and managed by Ms Otara Chandiram, herself a granddaughter of two eminent medical personalities of the past, ENT surgeon Dr HCP Gunawardene, and Cardiologist/Radiologist Dr HO Gunawardene. Having disposed of this successful venture, Otara is now preoccupied with animal welfare (in an honorary capacity), a subject close to her heart.
(This originally appeared in the Ceylankan)
To be continued next week

Sri Lanka is rising on the world’s travel radar – a jewel of the sun, drenched beaches, misty tea estates, and hidden waterfalls. Although Thailand dazzles with scale neon lights, bustling party islands and luxury resorts designed to impress, Sri Lanka offers something different, intimacy, authenticity and a luxury that doesn’t shout, it seduces.
As global travel surges and destinations vie for attention, the Deputy Minister of Tourism for Sri Lanka, Professor Ruwan Ranasinghe with deep roots in tourism studies, speaks about elevating Sri Lanka beyond its beautifully raw landscapes into a world class destination that embraces sustainability, technology and community empowerment. We spoke to him and asked what’s next for Sri Lanka and how the island envisions its tourism renaissance over the next few years.
 (Q) How do you foresee the tourism strategy direction for the next five years?
(Q) How do you foresee the tourism strategy direction for the next five years?
(A) Sri Lanka’s future tourism strategy is firmly anchored in sustainable and inclusive tourism. The focus is on balancing growth with responsibility: protecting natural and cultural assets while ensuring that communities across the island benefit directly. Diversification into wellness, eco-tourism, heritage, adventure, and rural experiences will be guided by evidence-based planning and inclusivity.
(Q) The key priorities for post pandemic recovery?
(A) Rebuilding trust with clear safety standards and transparent communication.
Inclusive growth by empowering small entrepreneurs and rural communities.
Sustainable practices in site management, energy use, and conservation.
Diversified demand targeting wellness, eco-travel, and long-stay visitors.
Digital transformation to modernize marketing and expand reach.
(Q) With Tourism booming in Thailand and Maldives, what is Sri Lanka’s position in the tourism landscape?
(A) Sri Lanka’s edge lies in offering a compact, diverse, and authentic experience— heritage, wildlife, tea, beaches, spa and wellness—all within short travel times. By positioning itself as a sustainable and inclusive destination, Sri Lanka appeals to travellers who value responsible tourism and meaningful cultural engagement, setting it apart from regional competitors.
(Q) What are your plans for sustainable and responsible growth for tourism?
(A) Sustainability is non-negotiable. Policies include carrying-capacity management, eco-certification, renewable energy incentives, and climate adaptation in coastal and hill-country zones. Inclusivity ensures that local communities share in tourism’s benefits, reinforcing resilience and equity.
(Q) How do we promote ecotourism, protect wildlife and marine ecosystems?
(A) Eco-tourism is being advanced through responsible visitor management, conservation partnerships, and community guardianship. Wildlife parks, marine ecosystems, and coastal zones are protected with stricter codes of conduct, while local communities are empowered as custodians and beneficiaries.
(Q) How can Sri Lanka showcase its position as a tourist destination?
(A) Sri Lanka presents itself as a sustainable, inclusive, and authentic destination. Live craft, cuisine, Ayurveda, and cultural showcases highlight the island’s unique identity, while digital tools ensure global buyers can connect directly with local providers.
(Q) How do we support small tourism entrepreneurs and rural communities?
(A) Inclusive tourism means empowering SMEs and rural communities with finance, skills, and market access. Homestays, village experiences, and community-based tourism routes are promoted to ensure equitable growth and authentic visitor experiences.
(Q) How do you predict the outlook for Sri Lanka’s tourism by 2030?
(A) By 2030, Sri Lanka envisions a tourism industry that is globally recognized for sustainability and inclusivity. Success will be measured not only in arrivals and revenue, but in conservation outcomes, community empowerment, and equitable regional development.
(Q) How will the role of technology and digital marketing help the tourist sector?
(A) Digital platforms and data insights will modernize Sri Lanka’s tourism, ensuring inclusive access for SMEs and smarter targeting of global markets. Technology supports transparency, efficiency, and sustainability, making tourism more resilient and competitive.
(Q) The impact of recent adverse weather and national disaster on tourism?
(A) Sri Lanka faced severe weather and a national disaster in the past months which inevitably disrupted parts of the tourism industry. Some destinations experienced temporary closures, and travel plans were affected. However, the government has acted swiftly: through the national budget and special allocations, resources are being directed to restore infrastructure, support affected communities, and stabilize the tourism sector.
Importantly, the industry’s resilience is evident. Stakeholders across government, private sector, and communities worked together with peaceful and strong dedication to minimize the damage. Recovery measures include targeted promotions to reassure international markets, rebuilding trust in Sri Lanka as a safe destination, and accelerating necessary upgrades.
This collective response demonstrates that Sri Lanka’s tourism is not only recovering, but doing so in a way that is sustainable, inclusive, and future-focused. The adversity has reinforced our commitment to building a sector that can withstand challenges while continuing to deliver authentic, safe, and memorable experiences for visitors.

The Prism story
 Tiesh is a luxury Sri Lankan jewellery house known for its high-end handcrafted pieces that combine contemporary design with traditional craftsmanship.
Tiesh is a luxury Sri Lankan jewellery house known for its high-end handcrafted pieces that combine contemporary design with traditional craftsmanship.
Recently Tiesh unveiled a fresh vision for contemporary luxury called the Prism Collection.
The Prism Collection is a jewellery line launched by Tiesh that draws its inspiration from the way light refracts and splits into rich, vibrant colours when passing through a prism.
The idea behind this collection is to capture the spectrum of light and translate it into wearable art -jewellery that highlights brilliance, colour and dynamic form.
This is an era where jewellery is more than mere ornamentation – where every piece tells a story. Launched to great acclaim at the brand’s elegant Colombo showroom, this collection is a radiant celebration of light, colour and refined artistry – a body of work that doesn’t just adorn but transforms.
Renowned for its dedication to excellence, Tiesh continues to uphold its legacy of producing jewellery that epitomises luxury, elegance and meticulous craftsmanship. Each Prism creation is thoughtfully designed and expertly crafted using the finest precious stones and the skill of master local artisans, reflecting the brand’s unwavering commitment to quality and detail.
Launched as a festive yet fashion-forward collection, Prism presents a curated selection of jewellery that aligns seamlessly with today’s modern aesthetic. Available in yellow gold, rose gold and white gold; the Prism Collection features an extensive range of designs, including rings, earrings, pendants, necklaces, bracelets, bangles and chains. Each piece is crafted to highlight colour, balance and wearability, appealing to the modern, trend-conscious jewellery lover.
With a proud legacy spanning almost three decades Staying true to this ethos, the Prism Collection places
Sri Lankan sapphires in the spotlight, celebrating their natural colours, textures and rarity. Speaking of the collection, Tiesh Co-Director Ayesh de Fonseka stated, “Prism was created in keeping with the times, contemporary yet timeless. In a time when the nation looks towards renewal, this Collection emerges as a symbol of hope and positive transformation. Reflecting light, colour and clarity, the collection embodies a sense of resilience and betterment. As proud Sri Lankans, we wanted
this collection to showcase the exceptional beauty of our local sapphires alongside other precious stones. These are statement pieces designed for modern lifestyles.”
The collection also embraces customisation, a signature element of the Tiesh experience. Clients are invited to select their preferred gemstones and personalise designs, resulting in truly one-of-a-kind creations that reflect individual style and expression.
With global gold prices reaching historic highs, fine jewellery has inevitably become heavier on the wallet Yet for discerning clients, the conversation is no longer about grams alone
Here customers can adjust stone size, setting style and medal choice to suit their budget. At Tiesh, you’ll notice another surprise – the after-care service such as polishing and maintenance.
The gold at Tiesh remains genuine and hallmarked. In collections such as the Prism line, gemstones and design architecture do most of the talking, while gold becomes the elegant framework rather than the bulk of the piece. In their collections the gemstones carry much of the visual richness. Instead of purchasing a heavy block of gold, the client invests in design, craftsmanship and beauty. So, when gold prices rise globally our jewellery doesn’t escalate at the same pace because gold is not the sole component defining the piece Ayesh pointed out
We create jewellery meant to live with the heavier, not just sit in a vault. At its heart, Tiesh remains more than a jewellery house; it is a family legacy shared by vision, trust and affinity with craftsmanship. And within every shimmering facet of Prism lies that story: a family craft containing to shine, generation after generation.
The Prism collection is now available at the Tiesh showrooms R A de Mel Mawatha Colombo 3.
Cinema, courage and conversation:
Renowned Indian actress Shabana Azmi brought candour, conviction and a lifetime of cinematic wisdom to the stage recently, in conversation with Sri Lankan author Ashok Ferrey at the HSBC Ceylon Literary and Arts Festival recently at Cinnamon Lakeside Colombo.
In a wide-ranging discussion that traversed five decades of cinema, feminism, censorship and cross-border politics, Azmi reflected on a career spanning over 140 films — dismissing the debate over whether the figure stands at 140 or 160 with characteristic wit. “One hundred and forty is good enough,” she quipped, setting the tone for an evening that blended humour with hard truths.
Ferrey opened the conversation with Ankur, the 1974 classic directed by Shyam Benegal, which marked Azmi’s debut and helped pioneer India’s parallel cinema movement. Azmi credited her formative years at the Film and Television Institute of India for shaping her craft, emphasising that acting is both talent and technique.
“Training polishes the diamond,” she said, rejecting the notion that acting can be mastered in a matter of months. Exposure to international cinema — from Japanese to French and Swedish films — deeply influenced her aesthetic choices, she noted, adding that her upbringing in a household steeped in theatre and poetry further shaped her artistic sensibilities.
Azmi spoke passionately about the delicate balance between emotion and technical precision required of an actor.
“You are in the moment, but you are also watching yourself,” she observed, describing the psychological demands of the profession. “Civilised behaviour expects you to control emotion. Acting demands the opposite.”
The discussion moved to Arth (1982), directed by Mahesh Bhatt, a landmark film in which Azmi portrayed a woman who refuses to reconcile with an unfaithful husband. The decision to let her character walk away — radical at the time — drew scepticism from distributors who doubted Indian audiences would accept such defiance.
“They said it wouldn’t run a single day,” Azmi recalled. Instead, it became both critically acclaimed and commercially successful, resonating deeply with women across India. She described how women began approaching her not as a star but in solidarity, seeking guidance.
“That’s when I realised I have a voice,” she said, marking the beginning of her active involvement in the women’s movement.
Azmi was unequivocal in her stance on patriarchy, describing it as deeply entrenched in South Asian society. While acknowledging that conversations have begun, she warned that social conditioning — including women’s acceptance of domestic violence — remains troubling.
The conversation turned to Fire (1996), directed by Deepa Mehta, a film that sparked controversy for its portrayal of a same-sex relationship between two sisters-in-law. Azmi admitted she took time to consider the role, anticipating backlash.
Encouraged by her husband, lyricist and writer Javed Akhtar, Azmi chose to proceed. The film was initially screened without incident before political groups vandalised theatres in protest. Yet she remains proud of her decision.
“If you can feel empathy for these two women, you can extend that empathy to others — another nation, race, religion or sexuality,” she said, underscoring her belief that art creates a climate of sensitivity where change becomes possible.
On ageing in cinema, Azmi expressed optimism. Unlike earlier decades when actresses were relegated to peripheral roles after 30, today’s industry offers space for senior actors.
She credited contemporaries such as Amitabh Bachchan — whose sustained presence in leading character roles has reshaped industry norms — for broadening opportunities.
The session concluded with reflections on cross-border tensions, prompted by a question about an India–Pakistan cricket match taking place concurrently.
Azmi offered a nuanced perspective, suggesting that while cricket fuels adrenaline, cultural collaborations — particularly film co-productions — could serve as stronger bridges between nations.
“People don’t have a problem with each other. Politics does,” she remarked, advocating for artistic exchange as a means of fostering understanding.
Throughout the evening, Azmi’s words echoed her lifelong belief: that cinema is not merely entertainment but a powerful vehicle for social transformation.
By Ifham Nizam

More than 1,500 Venezuelan political prisoners apply for amnesty

Six races, six golds – Klaebo’s historic Olympics

India, South Africa meet in the final before the final

Matara Festival for the Arts’ inaugurated by the Prime Minister

Showers or thundershowers will occur at most part of the Island after 1.00 p.m.

Only single MP refuses salary as Parliament details pays and allowances

‘Dates have the highest sugar content to fight Coronavirus’

Sunday Island 27 December – Headlines

#SundayIsland 17th December – Headlines

Sunday Island – 28th March

Sunday Island Headlines – 21 March

Sunday Island – 21st February – Headlines
-

 Business6 days ago
Business6 days agoMinistry of Brands to launch Sri Lanka’s first off-price retail destination
-

 Latest News2 days ago
Latest News2 days agoNew Zealand meet familiar opponents Pakistan at spin-friendly Premadasa
-

 Latest News2 days ago
Latest News2 days agoTariffs ruling is major blow to Trump’s second-term agenda
-

 Latest News2 days ago
Latest News2 days agoECB push back at Pakistan ‘shadow-ban’ reports ahead of Hundred auction
-

 Features6 days ago
Features6 days agoGiants in our backyard: Why Sri Lanka’s Blue Whales matter to the world
-
 Sports3 days ago
Sports3 days agoOld and new at the SSC, just like Pakistan
-

 News2 days ago
News2 days agoConstruction begins on country’s largest solar power project in Hambantota
-

 News5 days ago
News5 days agoIMF MD here