
News
Sri Lanka must sustain its health gains: malaria a case in point

by Prof. Kamini Mendis
Today, April 25, is World Malaria Day, and as many countries in the tropical world are laboring to control malaria and others racing towards the finish line to eliminate the disease, we in Sri Lanka are enjoying the prestige of being malaria-free. More importantly our people, possibly unknown to many of them, are benefiting from being free of a scourge, which destroyed lives and livelihoods, which took away most of our health budgets for insecticides, which stifled the cognitive development of our children and which greatly hindered Sri Lanka’s economic development for centuries past.
Today, we may be beleaguered by many health problems, not least, by the SARS-CoV-2 epidemic, but malaria is no more. The year 2012 saw the last case of malaria transmitted by a mosquitoe in Sri Lanka – a colossal achievement by any standards. And despite anxieties and worries whether the disease will return, the country has been kept free of malaria transmission for nearly nine years now, thanks to an exceptionally robust programme within the Ministry of Health, the Anti Malaria Campaign.
What we should be talking about today, though, is not the globally acclaimed achievement of malaria elimination from Sri Lanka, but whether and how the country can sustain its malaria-free status. A famed example etched in global public health chronicles is the historic achievement of Sri Lanka in 1963 of nearly eliminating malaria, and of the disease returning with a vengeance, to devastate the country for the next 50 years. This is a poignant reminder that malaria could still return.
Why so? The mosquito that transmits malaria is prevalent in parts of the country that were previously malarious. Even a new and highly efficient vector mosquito, which transmits malaria in India has been recently and inadvertently introduced into the country. Its implication is that if malaria returns to Sri Lanka it will affect cities as well as rural areas to which it was confined in the past. The threat of malaria becoming endemic again comes from imported malaria patients – those who acquire the infection abroad and return to Sri Lanka with the disease.
Most imported malaria infections are acquired in neighbouring India and African countries, and brought to Sri Lanka by such persons as business travelers, pilgrims, imported labour, and members of the armed forces and the Police Department who return from United Nations Peace Keeping Missions in malarious countries. Unless such infected persons are detected and treated without delay they could infect mosquitoes, and malaria could become endemic again – a possibility, that many health experts agree, must be averted at any cost.
What then must Sri Lanka do to remain free of malaria? It is to sustain a state-of- the art surveillance system to detect malaria patients returning from overseas and treat them without delay so that they will not infect mosquitoes and thereby transmit the disease to other people. Malaria can be easily diagnosed by testing a sample of blood using a rapid antigen test or by examining a blood smear under a microscope. Such diagnostic facilities are widely available throughout the country, and highly effective medicines are available to treat the disease.
Yet, simple as it might sound, the task of maintaining a rigorous programme of malaria case surveillance and treatment is fraught with challenges. This is because malaria is a rare and forgotten disease in the country today. Medical doctors fail, only too often, to test for malaria when a patient presents with fever. No blame to the physicians here, because there are so many other far more common causes of fever in the country – dengue, and a spate of other viral and bacterial infections to be explored as a cause of fever rather than malaria. But the clue to suspecting malaria is taking a history from the patient of recent travel overseas, which if present should place malaria high on the list of diseases to be tested for.
So, a combination of fever and having recently returned from overseas should be the signal to test for malaria. This is a message that the Anti Malaria Campaign is vigorously transmitting to its medical colleagues throughout the country – “when a patient presents with fever, ask for a travel history and test for malaria”. The Anti Malaria Campaign does far more than reminding doctors. It screens high-risk traveler groups for malaria throughout the country year round, and when a patient is detected it sets in motion a series of activities to ensure that the patient is cured, and that the infection has not spread to others in the country. it keeps track of the mosquito vector in all parts of the country and even controls it where necessary. It provides prophylactic medicines for travelers free-of-charge, and is the sole custodian of antimalarial medicines in the country, its staff being on call 24 hours a day seven days a week to keep the country malaria-free.
In truth, and the inspiration for me to write this article is that Sri Lanka has not had the most impressive record of sustaining its health gains, which have been made with enormous effort and major financial investments. We eliminated leprosy in 1995 but the disease has now returned to concerning levels in most parts of the country. We eliminated lymphatic filariasis a few years ago, but there is evidence that the disease may be lurking in parts of the country, with a risk of its transmission being resumed. Intestinal worm infestations, which sapped the nutrition of children for generations, have greatly declined in incidence, as have many other sanitation-related infectious diseases such as hepatitis. But, can we follow these achievements through to the point of extinction, and even more importantly, can we sustain the gains made?
“Out of sight, out of mind” is, unfortunately, a slogan, which most poor developing countries seem to live by when it comes to controlling diseases. They function on flimsy and short-sighted grounds that when a disease is not a health burden any more, the limited budgets for health are better assigned to other more prevalent health problems and diseases. Such thinking is clearly flawed on many counts: As careful studies and estimates have shown the price of preventing the return of malaria is only a mere fraction of the cost that Sri Lanka will have to bear if malaria returns to the country. It is estimated that the return on an investment of one rupee to prevent malaria will be 13 rupees in terms of the savings gained by preventing the return of malaria.
Developing countries must also desist a poorly informed but fashionable idea promoted in health circles even globally, of promoting the integration of dedicated disease control programmes into the general health services no sooner than the disease has been eliminated. Disbanding of these excellent programmes, the very ones which once eliminated the disease has been to the peril of countries as in the case of leprosy in Sri Lanka. Assigning the work of the leprosy campaign to the general health services too soon may not have been the most judicious of actions, and it may have contributed to the rapid return of the disease.
It is obvious that the workforce that was needed when a disease is highly prevalent would not be required to the same magnitude or degree of functionality when the disease is no longer a major burden. A carefully planned transition over time to shift work programmes from intervention delivery to surveillance, and share work time of staff with other related diseases has to be made, if it must, whilst maintaining a core of dedicated expertise on the disease at a central programme level.
The challenges of sustaining a malaria-free Sri Lanka and of keeping at bay other infectious diseases that we have successfully eliminated are many, but none that cannot be overcome by continued investment in, and maintaining the focus on, these diseases. It is an issue that falls broadly under the umbrella of “health security’, a term that has risen in importance with the SARS-CoV-2 pandemic, in the highly connected world that we live in. Today public health has come to the fore of our consciousness with the SARS-CoV-2 pandemic. Let our policy makers not forget that eliminating diseases is not the end-game, and that keeping those diseases at bay is as important as fighting other prevailing health problems.
About the author
Kamini Mendis is an Emeritus Professor and an international expert on malaria. She was instrumental in launching a Global Initiative to eliminate malaria in 1998 while working for the World Health Organisation Geneva. She has provided expert guidance to Sri Lanka and many countries on combatting malaria, and is gratified by the success achieved in the past few decades in many parts of the world. She continues to be engaged in advising the global and regional health communities and the Ministry of Health of Sri Lanka on the subject.
Latest News
Heat index is likely to increase up to ‘Caution level’ at some places in Eastern and North-central provinces and Monaragala, Hambantota, Jaffna, Mullaittivu, Kilinochchi, Vavuniya and Kurunegala districts

Warm Weather Advisory
Issued by the Natural Hazards Early Warning Centre of the Department of Meteorology at 3.30 p.m. 26 April 2025, valid for 27 April 2025.
The public are warned that the Heat index, the temperature felt on human body is likely to increase up to ‘Caution level’ at some places in Eastern and North-central provinces and Monaragala, Hambantota, Jaffna, Mullaittivu, Kilinochchi, Vavuniya and Kurunegala districts.
The Heat Index Forecast is calculated by using relative humidity and maximum temperature and this is the condition that is felt on your body. This is not the forecast of maximum temperature. It is generated by the Department of Meteorology for the next day period and prepared by using global numerical weather prediction model data.
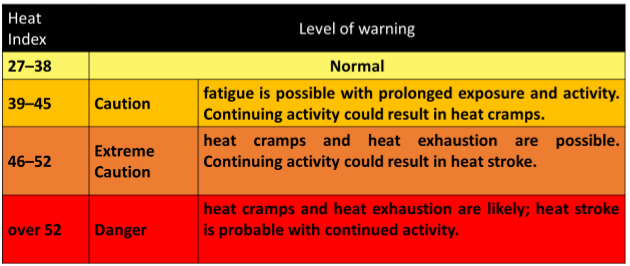
Effect of the heat index on human body is mentioned in the above table and it is prepared on the advice of the Ministry of Health and Indigenous Medical Services.
ACTION REQUIRED
Job sites: Stay hydrated and takes breaks in the shade as often as possible.
Indoors: Check up on the elderly and the sick.
Vehicles: Never leave children unattended.
Outdoors: Limit strenuous outdoor activities, find shade and stay hydrated. Dress: Wear lightweight and white or light-colored clothing.
Note:
In addition, please refer to advisories issued by the Disaster Preparedness & Response Division, Ministry of Health in this regard as well. For further clarifications please contact 011-7446491.

Minister of Foreign Affairs, Foreign Employment and Tourism, Vijitha Herath represented Sri Lanka at the funeral of Pope Francis on Saturday [26]

Former President Ranil Wickremesinghe will appear before the Commission to Investigate Allegations of Bribery and Corruption (CIABOC) tomorrow (28) over the statement he had made on MP Chamara Sampath Dassanayake, his lawyers have informed the Commission.
Accordingly, the former President will appear before the commission at 9.30am on Monday.
Wickremesinghe was initially summoned by the Commission to CIABOC on April 17 in relation to a statement he had made about the corruption case filed against NDF (gas cylinder) MP Dassanayake.
In response to the previous summons, Wickremesinghe had indicated that he is prepared to appear before the commission but requested a different date citing that his lawyers will not be available in Colombo during the New Year holiday period.
Accordingly, a new was provided and Wickremesinghe requested to appear before the commission at 09.30 a.m. on Thursday (April 25).On April 7, Wickremesinghe had said that MP Dassanayake withdrew the fixed deposits belonging to the Uva Provincial Council, over which he is now facing corruption charges, in accordance with a circular issued during Wickremesingher’s tenure as Prime Minister.
The former President questioned whether the MP’s arrest over the matter was in response to Dassanayake’s vocal criticism of the government in parliament.
The sitting MP is currently in remand custody for allegedly misappropriating a sum of Rs. 1 million of the Uva Provincial Council in 2016.
He was taken into custody on March 27, over three separate corruption-related cases.
The Colombo Magistrate’s Court previously granted bail in the cases filed against him but he remains in remand custody due to an order issued by the Badulla Magistrate’s Court.
According to the CIABOC, Dassanayake had solicited funds from three state banks, claiming they were intended to provide bags for preschool children in the province.
Two banks complied, granting him Rs. 1 million and Rs. 2.5 million, which were later transferred to his foundation account.
However, when a third bank refused to provide funds, Dassanayake reportedly retaliated by withdrawing the Uva Provincial Council’s fixed deposits from that institution.The CIABOC filed a case against the MP, citing the government incurred a financial loss of Rs. 17.3 million due to his actions.










-

 Features6 days ago
Features6 days agoRuGoesWild: Taking science into the wild — and into the hearts of Sri Lankans
-

 News5 days ago
News5 days agoOrders under the provisions of the Prevention of Corruptions Act No. 9 of 2023 for concurrence of parliament
-

 Features7 days ago
Features7 days agoNew species of Bronzeback snake, discovered in Sri Lanka
-

 News5 days ago
News5 days agoProf. Rambukwella passes away
-

 Business19 hours ago
Business19 hours agoPick My Pet wins Best Pet Boarding and Grooming Facilitator award
-

 News7 days ago
News7 days agoPhoto of Sacred tooth relic: CID launches probe
-

 Opinion6 days ago
Opinion6 days agoSri Lanka’s Foreign Policy amid Geopolitical Transformations: 1990-2024 – Part IX
-

 Features7 days ago
Features7 days agoSri Lanka’s Foreign Policy amid Geopolitical Transformations: 1990-2024 – Part VIII