Features
Testing for Covid-19: PCR and Rapid Antigen tests

By M.C.M. Iqbal
Associate Research Professor
Plant and Environmental Sciences,
National Institute of Fundamental Studies, Kandy.
iqbal.mo@nifs.ac.lk
Some basic facts about the two testing methods available to identify the Covid-19 virus, would help us understand the measures taken by the health authorities to control the spread of the virus. The virus that causes the Covid-19 disease (called SARS CoV-2) should be identified not only to manage patients but also to control the spread of the virus. As soon as the genome of the virus was made known by Chinese scientists in January 2020, tests were quickly developed to identify the virus. This test, popularly known as the PCR, is a chemical reaction performed in a PCR machine under very strict laboratory conditions to avoid contaminations. It is more accurately called rT-PCR, which stands for reverse Transcriptase Polymerase Chain Reaction. The discovery of this reaction earned Kary Mullis, a US scientist, the Nobel Prize for chemistry in 1993.
The genome of the virus is a long chain of four ‘letters’ of the genetic alphabet called RNA (most genomes, such as ours, are DNA). Using a combination of these letters, a complete set of instructions are available for the virus to gain entry into cells in our body, take over the machinery of the cell to make multiple copies of itself, which burst out of the cells to infect new cells. The genome consists of a very specific sequence of ‘letters’, which is peculiar to the Covid-19 virus. These ‘letters’ are chemicals called bases. The bases are codes for amino acids which are assembled into proteins. Scientists have isolated two fragments from the genome of the Covid-19 virus (the genome is nearly 30,000 bases long), which are unique to only the Covid-19 virus and not shared with RNA from any other organism. These unique fragments of the genome serve as a fingerprint for the Covid-19 virus. Using this as a basis, scientists have designed a test to unequivocally identify the Covid-19 virus.
By now, either you have personally experienced or seen on TV a trained healthcare worker attired in PPE inserting a plastic swab tipped with artificial cotton wool into the nose or throat. The swab has a long shaft, and it is gently scraped around the back of the nose or upper part of the throat (nasopharynx region). This can be  an uncomfortable experience particularly for children. This is the sampling process to conduct a test for the Covid-19 virus. The swab is immediately put into a tube with chemicals, sealed, labelled and sent to a laboratory.
an uncomfortable experience particularly for children. This is the sampling process to conduct a test for the Covid-19 virus. The swab is immediately put into a tube with chemicals, sealed, labelled and sent to a laboratory.
Of the many tests available, two are currently used in Sri Lanka. These are the PCR test and the Rapid Antigen Test. They differ in their sensitivity, specificity, cost and rapidity of results. The PCR test is conducted in a centralized laboratory, while the Rapid Antigen Test can be carried out on the spot.
PCR test
The PCR test is used to diagnose if a patient is infected or not with the Covid-19 virus. It is performed on patients with symptoms or on those who do not show any symptoms but are suspected of having an infection. It is vital that the test is highly sensitive and does not miss a patient infected with the virus (called a false negative result). The test should also be very specific to the Covid-19 virus; it should not diagnose a patient who is not infected with the Covid-19 virus as positive (called a false positive result). The PCR test is able to detect very low virus numbers in the patients. The results usually take around 12 to 48 hours.
Back to the sampling. The stuff on the swab needs to be cleaned. The RNA of the Covid-19 virus should be isolated from the rest of the other stuff that was scraped out from the back of the throat. There would be other bacteria and viruses, cells from our throat and mucus. These would have their own DNA and RNA. A combination of chemicals and detergents are used to clean up the sample and also to break open the Covid-19 virus to release its RNA, which is required for testing. Once this is done the sample is loaded into the PCR machine with another set of chemicals.
The PCR test is a very accurate and a nearly foolproof test for the presence or absence of the Covid-19 virus. It requires trained laboratory personnel, a modern laboratory, expensive chemicals and equipment, and time usually one or two days depending on the workload. Since PCR testing is very sensitive, it can detect the shedding of the virus from the patient even after the incubation period, and positive results can be given up to 17 days (see the figure). The incubation period is the time from exposure to the virus to onset of symptoms, which according to the WHO is on average 5-6 days but can be as long as 14 days. However, these PCR positive patients are no longer infectious and hospitalizing or quarantining them is a waste of hospital resources and agony for the patients. The WHO recommends that patients be discharged based on clinical recovery and not on a negative PCR. It is important to note that the PCR test detects the viral RNA fragments, and not the virus capable of causing infections. Thus, a positive PCR does not necessarily mean that a person has infectious virus and is capable of transmitting the virus to others.
Rapid tests for the Covid-19 virus
With a rapid surge in the numbers of infected persons, rapid tests are necessary to prevent the epidemic getting out of control. An on-the-spot testing method is necessary to decide if a bus load of people should be allowed to travel from a region with infected persons to a region which is relatively free of the Covid-19 virus. For this purpose, rapid tests have been developed that give results within 15 to 30 minutes. Similar to sampling for the PCR tests, here too a nasal or throat swab is mixed with chemicals on a paper strip to produce a colour reaction.
There are two different rapid tests for the Covid-19 virus. One is the Rapid Antigen test and the second is the Antibody test. Antigens are proteins found on the surface of the virus; being part of the virus a swab from the nose or throat will detect the virus. Antibodies are produced by our body against the virus and found in the blood, which needs a blood sample for testing. This test would tell us if our body has developed antibodies to combat the virus.
How does the Rapid Tests differ from the PCR?
The PCR test looks for a specific fragment of the Covid-19 viral RNA taken from the patient. Even if this is present in very small amounts the PCR machine multiplies them to high number of copies. The Rapid Antigen Test look for specific proteins on the surface of the virus. These proteins are called antigens, used in some vaccines and also recognized by our immune system to launch the defense against the virus. Unlike the PCR test, the antigens are not multiplied to sufficient levels for the test to detect the virus by the Rapid Tests. They act on the available load of the virus in the sample. The viral load in an infected person is the amount or number of virus particles in the body. Thus, if the virus load in the sample is low, the test can be negative – called a false negative. Obviously, these tiny virus particles cannot be counted; they are labelled as high, medium, or low viral loads. The progress of the viral load with time is shown in the figure.
Figure: Progress of infection, virus release and transmission by the patient, and periods of detection by PCR and Rapid Antigen Tests (RAT). Adapted from the references below. Days after infection are approximate.
Sensitivity of the tests
Sensitivity refers to how well a test is able to detect the virus – or specifically the RNA or proteins produced by the Covid-19 virus. The need for sensitivity is, however, different on what our objectives are. If the need is to diagnose a patient at the beginning of an infection cycle (see figure), then the gold standard is the PCR. If the need is to screen the population (many individuals), sensitivity is less of an issue: what is at stake is how infectious are the persons being tested. In other words, do these people have a high viral load with which they can transmit the virus? The RAT is ideally suited for this purpose: it detects high viral loads (hence infectious), many individuals can be screened, it is cheap, and results are available in 15 – 20 minutes. Thus, the primary need is not to determine if a single person with a small viral load can be accurately identified, but how efficiently infectious people can be detected in a population, who are capable of transmitting the virus to others. Thus, this would help the epidemiologist to isolate and remove infected persons and break the transmission chain. This could be people who are infected and also, importantly, those who are infected but do not show any symptoms, called asymptomatic, and those who are at the beginning of the infection cycle (see figure).
With PCR, there is a time frame from the point of sampling to the release of results during which the infection can spread. Infected persons can also spread the virus before symptoms appear. Those who do not show symptoms – asymptomatic – would also spread the virus. In this context, it is necessary to reduce the period between testing and confirmation of the results, which is not possible with PCR testing.
For the public it is important to note that a negative test results does not necessarily mean one is free of infection. If the test was performed at a point in the infection cycle (see figure) when the viral load is low the RAT would give a negative result.
Implementing the RAT more frequently, is an important tool for the epidemiologist to keep track of the spread of the virus and immediately implement isolation measures. An understanding of the infection cycle of the virus is necessary.
False negatives
What is of concern to the epidemiologist are false negative results – the person has the virus, but the test gives a negative result. This can happen if the Rapid Antigen test is done during the incubation period. During this period there may be insufficient viral proteins (antigen) in the nose or throat. The viral proteins are in sufficient amounts around 1 – 2 days before symptoms are seen.
False negatives, with PCR and RAT, can also result from incorrect sampling, if the swabs are not inserted properly and swished around in the nose and throat so that enough viral proteins or virus particles stick onto the swab. This can give a false sense of security or assurance to the person who may go around spreading the virus.
Implications for interventions
The roll out of effective vaccines would not necessarily end the pandemic. This is due to the challenges of successfully vaccinating the entire population and the resurgence of new variants with increased transmissibility, which was not anticipated earlier. In addition, there is asymptomatic transmission, and an overwhelmed health sector that is unable to attend to routine health needs of the people. Lockdowns and closures to reduce social interaction affects individual and government revenue. Hence, there is an urgent need for an early warning system on the spread of the virus in the population to deploy interventions by the state and prevent the uncontrolled spread of the virus. At present, monitoring of the virus spread is based on daily reports of PCR results, hospital admissions and random Rapid Antigen tests. This, however, does not reflect the prevalence of the virus in the broader community. The UK implemented a community-wide program to detect the resurgence of the virus at low prevalence in 2020 over six months (see Riley at al. in references). This was a real-time, country-wide population-based surveillance, that can be modified and conducted in Sri Lanka to monitor the Covid-19 virus and provide early warning. This could avoid sudden lockdowns and the inconveniences to the state, economy and the public.
References
McCartney M, Sullivan F, Heneghan C. Information and rational decision-making: explanations to patients and citizens about personal risk of COVID-19. Evidence-Based Med, 2020. [Epub ahead of print.], doi:10.1136/bmjebm-2020-111541.
Crozier, A., Rajan, S., Buchan, I., & McKee, M. (2021). Put to the test: use of rapid testing technologies for covid-19. bmj, 372. https://doi.org/10.1136/bmj.n208
He, X., Lau, E.H.Y., Wu, P. et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat Med 26, 672–675 (2020). https://doi.org/10.1038/s41591-020-0869-5
Mina, M. J., Parker, R., & Larremore, D. B. (2020). Rethinking Covid-19 test sensitivity—A strategy for containment. New England Journal of Medicine, 383(22), e120.
Guglielmi, G. (2021). Rapid coronavirus tests: a guide for the perplexed. Nature, 590(7845), 202-5.
Riley S. et al. Resurgence of SARS-CoV-2: detection by community viral surveillance. Science. 2021 6545):990-5.

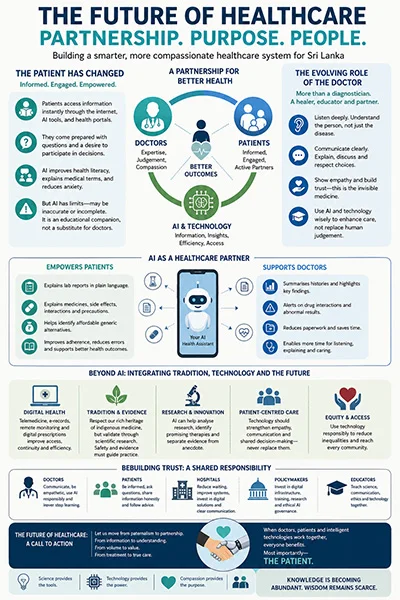
When Patients Become Partners:
The Waiting Room That Never Empties
 Picture a government hospital outpatient department on any weekday morning. Rows of plastic chairs fill before five o’clock. A mother holds a feverish infant against her chest, a folder of lab reports on her lap. An elderly man has travelled two-six hours by bus from his village. When she finally reaches the doctor, perhaps after three hours of waiting, the consultation lasts 2-4 minutes. A prescription is written in a hand that only the pharmacist has any hope of deciphering.
Picture a government hospital outpatient department on any weekday morning. Rows of plastic chairs fill before five o’clock. A mother holds a feverish infant against her chest, a folder of lab reports on her lap. An elderly man has travelled two-six hours by bus from his village. When she finally reaches the doctor, perhaps after three hours of waiting, the consultation lasts 2-4 minutes. A prescription is written in a hand that only the pharmacist has any hope of deciphering.
This is not a story of negligent unempathetic doctors. Most of those doctors are exhausted, processing 60 or 70 patients before lunch, doing the rough arithmetic of a system stretched well beyond its seams. Some patients jokingly compare busy clinics to a skilled coconut plucker moving rapidly from one tree to the next—not because doctors lack compassion, but because the system often leaves them little time to pause. In the private sector, the metaphor shifts — but only in its economics, not its pace. There, the imperative is to climb as many coconut trees as possible. What changes is who bears the cost of the hurry.
A legacy worth defending
Sri Lanka’s public health record is, by any regional measure, something to be proud of. Free healthcare at the point of delivery, a maternal/infant mortality rate that rivals middle-income countries far wealthier than us, these are not accidents. They are the product of generations of political will, professional dedication, and the idea that good health is a right, not a privilege.
The economic crisis of recent years sent a wave of trained doctors and nurses toward the Gulf, Australia, Canada and the United Kingdom. Specialists, who took a decade to train, departed within months. Meanwhile, the cost of private consultations has climbed beyond the reach of ordinary families, pushing them back toward an overstretched public system, or toward no professional care at all.
Patients who did their homework
Something else has changed, and it has changed faster than the system expected. The patient sitting across from the doctor today is not the patient of 10 years ago. She may have spent the previous evening consulting reputable online health resources or AI assistants, such as ChatGPT, to better understand her symptoms. He may have photographed his blood test results and run them through an AI tool that flagged an anomaly before the doctor mentioned it. They arrive with questions, about what additional tests are necessary for further diagnosis, about whether a test is strictly necessary, about what a particular reading on their lipid panel actually means for their life, especially when their life-styles are different. This is what educated, anxious human beings do when something threatens their health. The information age did not ask permission. It simply arrived.
The response from some doctors has been impatience, the feeling that an informed patient is a difficult patient. But the more productive response, increasingly voiced by thoughtful practitioners, is to see this shift as an opportunity. An informed patient is an engaged patient. An engaged patient is more likely to follow a treatment plan, more likely to return for follow-up, more likely to catch an error.
Authority to partnership
The old model of medicine was hierarchical by design. The doctor knew; the patient obeyed. That model had its logic, in an era when the knowledge gap between professional and layperson was absolute. That gap has not closed, but it has narrowed leading to a partnership.
There are doctors in Sri Lanka who already practise this way: arriving on time, spent 15-30 minutes with patients, contactable over the phone specially after a difficult procedure, for communicating plainly and without condescension. They are proof that the ideal is not utopian. It is achievable, which means the question is how to make it the norm rather than the exception.
Smarter, Not Harder
 This is where technology enters, not as a replacement for clinical judgment but as a tool for reducing the friction that currently exhausts both doctor and patient.
This is where technology enters, not as a replacement for clinical judgment but as a tool for reducing the friction that currently exhausts both doctor and patient.
Take the laboratory report cycle. A patient visits the doctor, is sent for tests, and a second appointment is required. A patient who arrives having already run those results through an AI-assisted tool is not trying to bypass clinical judgment or sidestep any genuine treatment decision. They are trying to eliminate a visit if they “know” that sole purpose is simply for an interpretation of the lab results. That second visit consumes time, money, efforts and transport. AI-assisted interpretation tools, not diagnostic systems, but educational ones, can give a patient a plain-language summary of their results (sometimes using Sherlock Holms’s theory of process of elimination to narrow down the possible causes) before they even walk into the consulting room. The doctor’s time is then spent on clinical decision-making, not on explaining what a haemoglobin or platelets count is.
Then there is the prescription. Illegible handwriting on a small slip of paper has long been a quiet patient safety hazard, and it is worth noting that AI tools have already begun helping patients and pharmacists decode what was written. But digital prescriptions go a step further: they eliminate the ambiguity entirely, and allow a patient to scan what they have been given, learn the name of each drug, understand what it does, and be alert to any side effects. This is not a challenge to the doctor’s authority. And when a patient discovers in the process that an approved generic equivalent costs a fraction of the branded price, they are empowered, not endangered.
Telemedicine, which got a reluctant push during the pandemic and has since retreated in public imagination, deserves a second look. Follow-up consultations for stable chronic conditions, blood pressure reviews, diabetes management, post-operative monitoring, need not always require a physical journey. The technology exists. The will to use it more widely is what remains to be mobilised.
Wisdom in herb garden
No conversation about healthcare in Sri Lanka is complete without acknowledging the parallel system that millions of people have never abandoned: traditional Hela medicine. Ayurveda, Siddha, Unani, and the vast informal knowledge embedded in village practice, these are not simply alternatives to modern medicine. For many Sri Lankans, they are the first resort.
The relationship between indigenous knowledge and scientific medicine has too often been one of mutual suspicion. Modern practitioners dismiss traditional remedies as unproven; traditional practitioners regard clinical trials as a foreign imposition. Neither position is adequate.
Consider Heen Bovitiya — known to botanists as Osbeckia octandra and to generations of Sri Lankan grandmothers as a trusted remedy for liver complaints and jaundice. Serious liver disease remains one of the conditions for which Western medicine offers no easy answer: its definitive treatment is a transplant — costly, risky, and followed by a lifetime of expensive immunosuppressant medication. Against that reality, a plant with pre-clinical evidence of hepatoprotective and anti-inflammatory properties is not a curiosity. It is a serious research priority. The studies so far are promising. They are also, as yet, large-scale clinical trials in humans have not been conducted, and questions of optimal dosage, mechanism of action, and drug interactions remain open.
The honest position is neither to dismiss the remedy nor to prescribe it uncritically. It is to say: this is a serious candidate for rigorous investigation, and Sri Lanka, which grows the plant, knows its traditional uses, and has the academic institutions to study it, is precisely the right place to conduct that research. AI tools that can process vast pharmacological datasets may accelerate that work considerably.
The future of healthcare should not be a competition between Western and indigenous medicine, but a commitment to evaluating all treatments by the same standards of safety, effectiveness, and quality.
Future Is Not a Machine. It Is a Better Conversation.
The fear that artificial intelligence will replace doctors is, at this stage, a distraction from the more important question. AI cannot examine a patient. It cannot feel the anxiety in a room. What it can do is handle the transactional, the look-up, the summary, the cross-reference, so that the human part of medicine can breathe.
The future worth working toward is not AI versus doctors. It is AI and doctors and informed patients, each contributing what they do best. The doctor could bring clinical expertise and the irreplaceable capacity for compassion. The patient brings self-knowledge, lived experience, and, increasingly, preparation. The technology brings tireless availability and pattern recognition at scale.
What we measure matters. A consulting room’s success should not be counted in patients seen per hour. It should be counted in patients who leave feeling informed about their condition, respected as partners in their own care, reassured that someone is genuinely attending to them, and confident about what to do next.
The Thing Patients Remember
There is a truth that experienced nurses know, that the best doctors quietly understand, and that patient experience research consistently confirms: patients may forget the prescriptions. They may forget the name of the drug, the dosage, even the diagnosis. But they rarely forget how they were treated, pleasant or rude.
They remember the doctor who looked up from the desk. The one who said, “That’s a good question.” The one who spent two extra minutes to listen, drawing a small diagram to explain where the problem was. They remember being seen, not just examined, but truly seen, as a person rather than a case number.
Sri Lanka has those doctors and nurses, in every district, in every ward, working against the odds. The task now is to build a system worthy of them, and of the patients who place their lives, without much choice in the matter, in their hands.
Technology may transform medicine. Artificial intelligence may transform diagnosis. Digital health may transform hospitals. But trust will always define healing.
(The writer, a senior Chartered Accountant and professional banker, is Professor at SLIIT, Malabe. Views expressed in this article are personal.)
By G. Usvatte-aratchi
(B.A. (Cey.); Ph.D. (Cantab.))
Eric came to Ramanathan Hall in June, 1954, from Mahinda College, Galle, with much celebrity. He was one of the youngest in the freshmen class. In Galle, in the 1950s, there were several schools where students studied to enter the University of Ceylon: Mahinda, Richmond and St. Aloysius’. Mahinda College, under Principal E .A. Wijesuriya, had become a powerhouse, sending brilliant students to the University of Ceylon. Siri Gunasinghe was on his way to stardom, shining brightly in Sinhala poetry, fiction and drama, besides his main academic interest in arts history. Eric, in time, shone with no less brilliance in a wider constellation, spreading enriching light onto the lives of millions of people in this land. I was privileged to be his friend.
We were two among the 20 students who studied for the Economics Special degree, 1958. His teachers included A. J. Wilson and I. D. S. Weerawardena, both outstanding academics who excelled as scholars as well as teachers. His fellow students were Mirani Perera (Secretary, Central Bank), Dharmasiri de Alwis (later Dharmasiri Senanayake), (Secretary of the SLFP, a Minister in Sirimavo Bandaranaike’s government, and a smart politician), Wijeratne (GATT, Geneva) and several others. I followed a different specialisation and chose a different career.
In 1959, Eric joined the public service as a member of the elite Ceylon Civil Service. It was usual for a few of the smartest students in the university, each year, to compete for a few places in the Ceylon Civil Service and Eric was one of them. A few who preferred an academic career stayed back in the university; in our year Hemapala Wijewardena, a truly brilliant man who rose to be Professor in the Department of Sinhala in Colombo, was one such.
In 1955 (or 1956?) N. K. Sarkar from Calcutta, who taught us statistics, and S. J. Tambiah, who later became Director of the Peabody Museum and a world-renowned anthropologist at Harvard, undertook a survey of five villages in Patadumbara, as they were interested in changes in our society and agrarian relations in that part of the country. The findings of that Survey, published by the University of Ceylon Press as ‘The Disintegrating Village,’ were seminal, in effect. The anthropological studies of Edmund Leach (of Cambridge), Pul Eliya and later, the prolific work of the anthropologist Gananath Obeysekera (of Princeton) were deeply influenced as to the methods of research and subject matter thereof. Eric and I were teamed together to visit families and fill questionnaires. One morning, we noticed that the families we visited lived in thatched houses, most of which had no lockable doors. Out of curiosity we gently inquired why they did not lock their doors. They in return asked us why would anyone want to burgle homes where there was nothing to steal.
Eric married Trixie soon after she graduated having wooed her after she came to Peradeniya. Trixie and her sister Dulcie lived with their aunt in a house immediately next to the Boys’ Hostel of the Hikkaduva Central School, where we juniors were housed. Their brother Derek was at school (Richmond?) in Galle and later joined the Army as an officer. Sarachchandra started rehearsing students to act in Maname in 1956 and Trixie was selected to the small choir. Eric immediately became a keen, avid aficionado of drama and missed hardly any rehearsal. He made sure that he stayed close to Peradeniya after graduation by securing a position as a teacher in Dharmaraja College, Kandy. Their four children brought distinction to themselves and their parents. Nishantha, a scientist, who taught at Jayewardenepura, and later at State College, Pennsylvania, was most remarkable in her devotion to the care of her son; Manjula won first class honours in economics at Colombo and obtained a higher degree in London; Varuna, who stayed back in Colombo with his father and Sanjaya with a Ph.D. from Yale and was a Professor of Economics at Bard College in upstate New York. Apart from their intellectual brilliance they honoured themselves and their parents by maintaining lives of the highest integrity.
Eric was the Government Agent in Trincomalee for several years and lived in a bungalow in a sprawling compound with the beach as one boundary. Deer freely roamed in his compound. One summer, which we spent in Colombo, my family were their guests. Trixie and Eric were perfect and graceful hosts and the children had a whale of a time which they recalled for many years. Varuna was the leader of the gang and we had one photograph (from those days of cumbersome photography) of them going in a procession on the beach. As the children grew up to go to school, Eric came to live in Wijerama Mawatha, Colombo.
Among the episodes in his work that Eric talked about, two stand out in my memory. Eric worked in an office of Prime Minster of Sirimavo Bandaranaike, with W. T. Jayasinghe as the Permanent Secretary. Martin Wickremasinghe’s novel Bava Taranaya was published in 1973 and, immediately, there was widespread agitation among some Buddhists because the account in the novel of the life of Siddhartha Gautama differed very much from the orthodox accounts that had grown over more than a millennium. Prominent learned bhikkhu led the charge, among them Yakkaduve Pragnarama of Vidyalankara and Henpitagedera Gnanaseeha. Bhikku were one of the highly influential parts of the constituency of SLFP and Gnanaseeha was one of the most prominent among them. Bandaranaike was a most astute politician and could not be rushed into any ill-advised action. Jayasinghe informed Eric that the Prime Minister wanted a report on the book to help her make up her mind on the question. During a weekend, Eric read the novel and his report was handed over by Jayasingha to the Prime Minister. Someone wrote an evaluation of Bava Taranaya, a few days ago in the Lankadeepa.
When Eric was in Trincomalee, Amaradasa Gunawardena (Ramanathan,1958, Sinhala Special) was in Polonnaruva. One year there was a severe drought which threatened to ruin the rice crop in Trincomalee while the reservoirs in Polonnaruva were brimful. There was much agitation and rice growers urged politicians and public servants to seek solutions. Eric spoke to Amaradasa and went to meet him at the border. Hope ran high in Trincomalee. In the evening, when he returned to his office, Eric was garlanded and there was much jubilation. He continued to be feted the whole week. Many prominent citizens and savvy politicians urged Eric to contest the Trincomalee seat in Parliament. There were precedents when successful Government Agents had successfully entered politics from their districts. Eric limited himself to become a distinguished public servant.
Eric’s work at the Ministry of Education made a lasting impression on his mind. Of the many problems he handled as a senior public servant, nothing interested him as school education did. I had learnt about medieval universities, for the first time, in a course of three lectures that Fr. S. I. Pinto delivered in my first year at Peradeniya. Eric was not in that course. I read Rashdall’s three-volume definitive study on that subject and has never stopped reading it. I came back to live in Colombo in 1996, with a commitment to contribute to educating the public on economics and social problems in the country and selectively elsewhere. About that time there were a few scholars actively studying school education: Swarna Jayaweera, S. Sanderasegaram, Ariyadasa de Silva (all in Colombo), Chandra Gunawardana (Open University) and G. B. Gunawardana (NIE). They were mostly students of the illustrious professor J .E. Jayasuriya (Peradeniya). They provided a small audience with whom we could share our interests. Both Eric and I delivered lectures in honour of J. E. Jayasuriya. Eric used to pick up Varuna’s daughter from the British School which was 10 minutes’ walk from my home and Eric, not infrequently, stepped in. We often chatted on subjects that interested us. After a while, Eric suggested that we might collect a few more people to join in the conversations. Effortlessly, we went back to Peradeniya days and invited Haris de Silva (historian and Government Archivist), W. M. K. Wijetunge (historian and Professor) K. S. E. Jayatilaka (Economic Statistician and Deputy Governor, Central Bank) and Mettananda (Ministry of Education).
We pompously called ourselves the Education Research and Study Group (ERSG) and met in my porch. Each of us contributed an equal sum of money, which did not amount to a lot but we managed it carefully. The only resources we received from outside were the services of a professor from a German university, which the Goethe-Institut, Colombo paid for. We mostly chatted about what we had read and mused about in the previous fortnight and our reactions to educational matters that had come up. We discussed both school and university education. Our discussions inspired Eric to write the short book, ‘Politics of Education Reform and other Essays’. When we had sufficient material, we called a public seminar and were pleasantly surprised that we had an audience. We congratulated ourselves when the ministry changed a policy or other course of action in reaction our presentations in the press. We disbanded ourselves when some of us pre-occupied themselves with other matters.
We celebrate Eric’s life and work. He carried with himself the education and training that he received from Mahinda College, Galle and the University of Ceylon. With quiet efficiency, that was characteristic of much of the Civil Service, Eric worked at the highest levels in management when institutions in the new state Ceylon were yet in a formative stage. As that state matured into Sri Lanka, the purposes and procedures in many of those institutions frayed and their energy sapped. The commitment and the enthusiasm that Eric exhibited are high value assets with which to start their reformation and revitalisation.

Sri Lanka is witnessing the dismantling of the culture of impunity that dominated public life for decades. This is happening through the courts, police investigations and legal process. It is not an easy task and requires strong leadership as it is generating strong resistance. The ongoing revelations about the nexus between politicians, including those at the highest levels, and criminal networks show that the government’s electoral mandate with regard to corruption and crime is now being translated into action through the legal system. The vote of the people at the last national elections was for a corruption free country and an end to the climate of impunity that had prevailed for decades. They voted for a system change that would replace impunity with accountability under the rule of law. They expected those who had looted the country and brought it to the point of bankruptcy to be held accountable through the due process of law.
The cases that are being investigated by the police, in tandem with the Attorney General’s Department, and adjudicated by the judiciary are based on hard evidence. Much of the evidence that is now receiving publicity had been available several years ago and had even entered the legal process. In the past those cases failed to reach fruition. Investigations lost momentum, prosecutions failed to marshal the available evidence and many cases were dismissed, some on technical grounds. Between 2019 and 2024, a total of 102 cases were withdrawn from the courts by the government authorities. The public knew, or strongly believed, that corruption and serious crimes had taken place. The inability to establish wrongdoing before a court of law and hold those responsible accountable created a climate in which political power appeared to provide protection from legal accountability.
A countrywide study titled Factors Guiding Voter Preference in Elections in Sri Lanka was commissioned by the National Peace Council prior to the 2024 elections under the European Union funded project Active Citizens for Elections and Democracy and conducted by researchers Dr Mahesh Senanayake and Ms Crishni Silva of the University of Colombo. It found overwhelming public support for accountability and good governance. While 93 percent of respondents identified resolving the economic crisis as their foremost electoral concern, an equally striking 83 percent said they prioritised candidates committed to fighting corruption. The mandate given to the government can, therefore, be interpreted to mean to restore integrity to public life and end the long standing culture of impunity.
Different Approach
Today, it can be seen that the police, the Commission to Investigate Allegations of Bribery or Corruption, the Attorney General’s Department and the judiciary are approaching matters of impunity in respect of corruption and crime in a manner that is markedly different from the past. Several persons who formerly occupied high office have now been subjected to due legal process and, in a number of cases, convicted after judicial scrutiny at different levels of the court system. This is an important difference from earlier years when cases involving politically prominent persons frequently failed to proceed or collapsed before reaching their conclusion. The strength of the present accountability process lies not only in the convictions that have been secured but also in the growing public confidence that no one is above the law. It is in this context that reports of a government proposal to extend by two years the retirement age of judges of the Supreme Court and the Court of Appeal have generated support from those who wish to see the present accountability process continue and opposition from those who see it as an attempt to influence the judiciary.
Many countries have increased judicial retirement ages in recognition of longer life expectancy and the value of retaining experienced judges. This has not only been limited to the judiciary but also the academia and the public service. However, the controversy in Sri Lanka is due to the context and as the proposal for an extension of the period of service of judges of the superior courts comes at a time when the courts are hearing politically significant corruption and criminal cases. The Bar Association of Sri Lanka has taken the lead in questioning the proposed constitutional amendment. The BASL has stated that it “notes with grave concern” reports that the government is considering increasing the retirement age of judges of the Supreme Court and the Court of Appeal. It has warned that extending the tenure of sitting judges at this point of time is likely to be viewed by the public as an attempt to interfere with the independence of the judiciary.
The main issue raised by the BASL is therefore one of preserving public confidence in the administration of justice. A discussion organised by the BASL also highlighted that this issue has implications beyond Sri Lanka. Representatives of the Commonwealth Lawyers Association and LAWASIA acknowledged that many countries have increased the retirement age of judges in recognition of greater life expectancy and the value of retaining experienced judges. Their concern was not with increasing the retirement age itself but with changing the tenure of sitting judges while politically significant corruption cases are before the courts. In such circumstances, even well intentioned reform could create a public perception that the judiciary is being influenced to take forward the government’s mandate in a partisan manner.
Maintain Confidence
The challenge before the government is to preserve two equally important objectives. The first is to continue implementing the people’s mandate to hold the corrupt and those responsible for grave crimes accountable before the law. The second is to ensure that nothing is done which could diminish public confidence in the independence and impartiality of the judiciary that is entrusted with carrying out that responsibility. The strength of the present accountability process lies in the confidence it has generated among the public that investigations, prosecutions and judicial decisions are being made according to law as in the convictions that have been secured. Sri Lanka has come a long way from the days when politically sensitive cases rarely reached a successful conclusion. It would be unfortunate if doubts regarding the independence of the judiciary were to overshadow what has otherwise been a significant institutional achievement.
In the face of the concerns expressed by the BASL, opposition political parties and international legal organisations, it would be prudent for the government to widen the discussion on the proposed amendment. If there is a compelling case to increase the retirement age of judges of the superior courts, that case should be placed before the public and parliament and debated openly. Such a constitutional amendment should not rest solely on the government’s parliamentary majority, even if it has the numbers to secure its passage. Simply utilising the numbers that the government on its own to make changes to the constitution will not increase its legitimacy or credibility. Those values will be strengthened if they were preceded by public consultation and supported across party lines in Parliament. Bipartisan political support can be expected from those in the opposition, of whom there are many, who have shown an inclination to practice responsible politics in the national interest.
The people voted not only to change a government but to change a system. They expected those who abused public trust to be held accountable through institutions that commanded public confidence. That expectation is beginning to be fulfilled. It should not be placed at risk by constitutional change that lacks broad public acceptance. If the government believes there is a compelling case to extend the retirement age of the judges of the superior courts, it should first make that case to the people and seek bipartisan support in Parliament with those in the opposition who are also sincere about anti-corruption and good governance. The challenge is to protect the independence of the judiciary while ensuring that no one is above the law. Overcoming this challenge is the surest way to make Sri Lanka’s transition from a culture of impunity to one of accountability a lasting one.
by Jehan Perera

President chairs 2027 Pre-Budget talks on Agriculture Ministry

Committee Appointed to investigate unrest at Negombo Prison

Archer, Tongue hand India their biggest T20I defeat

“Badhu Shakthi 2026” National Tax Week begins

Renovated Narahenpita Railway Station reopens to the public under the ‘Dream Destination’ initiative

High-scoring draw gives West Indies rare series win

‘Dates have the highest sugar content to fight Coronavirus’

Sunday Island 27 December – Headlines

#SundayIsland 17th December – Headlines

Sunday Island – 28th March

Sunday Island Headlines – 21 March

Sunday Island – 21st February – Headlines
-

 News4 days ago
News4 days agoSingapore-based Buddhist monk marks nearly four decades of humanitarian service
-

 News5 days ago
News5 days agoFreedom 250: US Embassy celebrates America’s 250th Independence Day through magic of American cinema
-

 News5 days ago
News5 days agoCIABOC to question Harak Kata on Rs. 200 mn bribery allegation
-

 News6 days ago
News6 days agoSLAF conducts successful rescue mission under UN command in Central African Republic
-

 News3 days ago
News3 days agoAI concerned over proposed SL military deployment in Haiti
-

 News5 days ago
News5 days agoUNEP support pledged to strengthen Sri Lanka’s Environmental Priorities
-

 Business6 days ago
Business6 days ago‘Dialog Air Fibre powers a new era of Ultra Fast Home WiFi’
-

 Features4 days ago
Features4 days agoThe NPP’s New Challenge: Balancing Easter Lawfare and Economic Welfare