Features
History of Leprosy in Sri Lanka: Saga of three millennia

By Ifham Nizam
Nearly 1500 new patients with leprosy are diagnosed each year. Almost 50 percent of them are residents of four districts, Colombo, Kalutara, Gampaha and Batticaloa. Some areas in the northern, Uva and Central provinces have very few cases and may be considered areas that have “eliminated” leprosy in the true sense, says a senior medical officer.
Dr. Indira Kahawita, Consultant Dermatologist, Anti Leprosy Campaign, Sri Lanka, told The Island that 10 percent of the patients are children below 14 years of age.
“This is an indication of ongoing transmission within the country. About seven percent of the patients have permanent nerve damage at the time of diagnosis. This means there is a delay in diagnosis,” Dr. Kahawita stressed.
Excerpts of the interview with Dr. Kahawita:
* Does leprosy have a long history in Sri Lanka?
Yes, the history of leprosy is as long as the history of the country itself. There is evidence from the ancient medical books, as well as from the chronicles on history. But one need to remember that the disease wasn’t called leprosy then.
In some of my descriptions I have used the terms leper and asylum. These words are used only in the historical context. In the modern world these words are considered discriminatory and are not used.
* Then how is it possible to come to conclusions?
Firstly, some ancient books on medicine, written in the Anuradhapura era, describe symptoms and signs of skin diseases, similar to leprosy. The most notable among them are; Sarartha Sangrahaya” by the Surgeon King Buddhadasa in the 5th century, “Yogarnavaya”, written by Bhikku Buddhaputhra in the 12th century, and “Bhesajja Manjusawa”, written by “Paspiruvan mula/head of five piriven” Bhikku in the 13th century. All these books describe several presentations of “kushtha” that are identical to leprosy. The same is true for the well known Ayurvedic books, “Charaka Sanhithawa” and “Susrutha Sanhithawa”.
After going through these texts very carefully, one can deduct that the word “kushtha” was an all-encompassing term similar to the word ‘rash’ in today’s context, and that leprosy was definitely one of them. Both the Sushrutha and Charaka Sanhitha give almost identical descriptions of “kushtha poorwa roopa”or symptoms of “kushtha”. The absence of sensation, absence of sweating, paraesthesia, goose bumps, unusual pain in the wound (neuropathic pain), ulcers that occur easily and last longer and numbness of organs have been described as symptoms of “kushtha”. Several types of “kushtha” described in the books written in Sri Lanka are identical to the individual features of leprosy.
Secondly, the “Mahawansa” narrates how king Buddhadasa cured a leper of his deranged mental condition when he used abusive language at the king in the marketplace. The statue “Kushtaraja Gala” in Weligama, is now established as an Avalokitheswara bodhisatva. Bodhisatva worship was used for relief from illness and it is believed that lepers of the South worshipped this statue seeking relief.
* What about the legend of the “lion” and Suppa Devi and the
beginning of the Sinhala race?
If one were to think of a medically plausible explanation for the lion, the most suitable would be a well-built young man with lepromatous leprosy who had who had fled to the jungles due to his disease. In fact, the changes in the face in lepromatous leprosy are termed “leonine facies” – face of a lion.
If this is the case, the fact that their offspring were later received at the Royal Court confirms that discrimination against those affected was minimal at that time.
* Was leprosy a dreaded disease in the ancient past?
It is difficult to say that persons affected were not discriminated at all. But the story of Sinhabahu and the fact that the leper who abused king Buddhadasa was able to do so in the market place suggest that those affected were allowed to live freely within the society. The Thripitaka contains the “Suppabuddha Kutti suttha” narrating the story of a person affected who sat in the audience with the others to listen to the preachings of the Buddha who gained enlightenment as the Buddha preached aiming him specifically. Even the bioarcheological work in the Indus valley have shown evidence that there was an empathetic attitude towards those affected.
* What was the status of leprosy in the colonial period?
Even though there are no written records from the Portuguese period, many documents from the Dutch period give details about the status of leprosy. The disease was prevalent in the areas under the Dutch rule and the rulers had started to segregate those affected in order to prevent further transmission. Initially, they were banished to Tutucorin, in India. Later the Dutch East India company allocated funds to build the leper asylum in Hendala. Leprosy was a major health problem in the Dutch era and the officials had been prompt in tackling the situation.
The highlights of the British period are the lepers ordinance no 4 of 1901, the building of the leprosy hospital in Manthivu, off Batticaloa, and the introduction of the early treatments for leprosy. The Lepers Ordinance imposes compulsory segregation of those confirmed to have leprosy. Since all those diagnosed could not be housed within the leprosy hospitals, home quarantine was also practiced.
* What is the status of leprosy hospitals now?
The hospital at Hendala houses patients who were admitted several decades ago. They are there as they have lost family ties due to long separation. In its prime the hospital had boasted of around 700 patients, the best possible medical care and nursing support of religious sisters from many sects. The eminent doctors had done immense service to leprosy care in the country and some have even been honoured by the British empire.
The hospital at Manthivu was opened in 1921 due to the logistic difficulties in transporting patients from the East to Handala. It was decided to close the hospital and transfer 38 patients to Hendala due to safety concerns during the civil unrest in 1996. Two patients who had refused to be moved still remain there.
A leprosy colony, meant for able bodied patients to undergo inpatient care while being economically independent, functioned at Uragasmanhandiya, in the Galle district, for a short period, from 1952 to 1963.
* Why were patients segregated?
There was no effective treatment at that time. In fact, in the Dutch period, it wasn’t even known that leprosy was caused by a bacterium. But it was accepted that spread of the disease could be contained by removing those affected from the community. Initially, segregation was voluntary but after 1901 all patients diagnosed were under segregation, irrespective of their status.
* Does it mean that there was no treatment whatsoever during those days?
The initial treatment options were oils extracted from certain plants as external applications. During the late 19th century, two oils; gurjun oil extracted from the plant Dipterocarpus turbinatus and chaulmoogra oil extracted from the plant Hydnocarpus wightianus were used as massage oils.Chaulmoogra oil became the mainstay of therapy in the 1920s, when better techniques of preparation made it possible for the oil to be used as an oral drug and an injection. But the injections were painful and the response to treatment was around 50%.
With the introduction of a group of drugs called sulphones in the 1930s the treatment took a new turn. By the 1950s dapsone, a better and newer sulphone, was used as monotherapy (single drug therapy) for long periods. Since the organism has the tendency to alter itself to escape the effects of one antibiotic resistance to dapsone was soon identified.
* When was effective treatment for leprosy available in Sri Lanka?
In 1982 the World Health Organization (WHO) introduced a combination of antibiotics called the Multi Drug Therapy (MDT). Sri Lanka started using the MDT island-wide in 1983 and approximately 100 000 patients have been treated with MDT over the past 40 years. There are two types of treatment, paucibacillary (PB) given for six months for those with less severe disease and multibacillary (MB) given for 12 months for those with the more extensive form of the disease. The treatment is provided free of charge by the WHO and is available at government hospitals island-wide. The treatment can be used safely even in pregnant and lactating mothers and children.
*There were popular awareness programmes in the past. Were they effective?
The most effective awareness programme was conducted in the late 1980s with messages about the signs and symptoms of leprosy and that leprosy is curable over all available media. The two teledramas, “Ella langa walawwa” and “Ira Paya” were very effective in taking the message about leprosy to the masses. With improved awareness, the number of patients identified almost trebled in 1990. Many patients presented for treatment by themselves. Since 2000, approximately 1500 to 2000 new patients have been diagnosed each year. There was a drop in the detection of new cases after the COVID-19 pandemic, the Anti-Leprosy Campaign has started a social marketing programme over mainstream and social media called “LIFE Sri Lanka” in 2022.
* Has Sri Lanka eliminated leprosy?
When the WHO introduced the goal of “Eliminating leprosy as a public health problem” in the 1990s the parameter used was “less than one patient with leprosy per 10,000 population”. This highly technical point was not understood even by some healthcare workers. So, the message that was accepted by the public was that “Sri Lanka has eliminated leprosy, or leprosy is no longer present in Sri Lanka”. This misconception may have led to the missing of the diagnosis in many patients. If we look at the statistics for leprosy in Sri Lanka for the past 60 years, we can see that the numbers detected in the country have been within the WHO’s parameters even in the 1960s.
* What is the status of leprosy in Sri Lanka now?
Approximately 1500 new patients with leprosy are diagnosed each year. Almost 50% of them are residents of four districts, Colombo, Kalutara, Gampaha and Batticaloa. Some areas in the northern, Uva and Central provinces have very few cases and may be considered areas that have “eliminated” leprosy in the true sense
10% of the patients are children below 14 years of age. This is an indication of ongoing transmission within the country. About 7% of the patients have permanent nerve damage at the time of diagnosis. This means there is a delay in diagnosis.
*What measures have the authorities taken to control leprosy in Sri Lanka?
The Anti Leprosy Campaign (ALC), the organization in charge of leprosy control, is using a multi-pronged approach to improve awareness about leprosy, both among healthcare workers and the public. The ALC has mapped the country into risk areas according to the WHO’s most recent recommendations and is now in the process of using GIS technology to identify areas with high disease burden and to target those areas for awareness and case detection.
Our aim is to use strategies specifically suited for each area of the country so that all possible cases are diagnosed and started on treatment early. Since treatment of cases and minimizing the reservoir of infection is the only effective method of disease control for leprosy, we are hopeful that the improved strategies will take the country towards zero leprosy or true elimination of the disease.

(Part I of this article appeared in The Island yesterday.)
An examination of how some of the other countries have institutionalised mediation to address the problem of laws delays shows that an array of institutional devices have been adopted to provide for mediation not only as a voluntary option but also in some jurisdictions, as a mandatory requirement prior to litigation, to respond to serious issues of delays due to congestion in courts.
In the UK , in March 1994, the Lord Chancellor commissioned Lord Woolf to review the Rules of civil procedure with a view to improving access to Justice, reducing the cost of litigation and removing unnecessary complexity. The resulting Access to Justice Report (1996) triggered a series of reforms to improve the civil justice system primarily through the civil procedure rules (1999) which articulated that its overriding objective is to enable the court to deal with cases justly and at proportionate cost. In 2023, the Court of Appeal judgment in Churchill v. Merthyr Tydfil County Borough Council [2023] EWCA Civ 1416, decided that English courts do have the power to stay civil proceedings for, or order, parties to engage in mediation or another non-court- based dispute resolution process. The Rules were thereafter amended in 2024 to provide for the use of alternative dispute resolution (ADR) more proactively. These included rules that recognied that –
* promoting or using ADR is a means of achieving the overriding objective;
* the court has a duty to actively manage cases to further the overriding objective, including by ‘ordering or encouraging the parties to use, and facilitating the use of, alternative dispute resolution’ and ‘helping the parties to settle the whole or part of the case’
* in deciding a costs order, a court will have regard to all the circumstances of the case, including the conduct of the parties, including whether a party failed to comply with an order for ADR or unreasonably failed to engage in ADR.
An ADR pledge made by the UK Government in 2001 was renewed in 2011, by the Dispute Resolution Commitment (DRC) requiring departments to use mediation, arbitration and conciliation. At that time, the then Justice Minister Jonathan Djanogly said: ‘I believe that government should be leading by example by resolving issues away from court using alternatives which are usually quicker, cheaper and provide better outcomes. We want people to see court as a last resort rather than a first option, and cut down on the amount of unnecessary, expensive, painful and confrontational litigation in our society. In many cases methods like mediation are simply a common sense solution which benefits everyone involved. Although they will not be suitable in every case, they are already saving taxpayers millions every year and can save much more.’
The judicial dicta on the power of the courts to order mediation and the imposition of costs on even a successful party for unreasonable refusal to mediate, provides clear acceptance of a pro mediation approach by the UK courts.
In the USA , the discussion on the need for alternatives was raised in a speech made in 1906, by Roscoe Pound, a relatively unknown legal academic at the time, addressing the annual meeting of the American Bar Association (ABA). The title of his address was “The Causes of Popular Dissatisfaction with the Administration of Justice.” He critiqued the American legal system and charged that it was riddled with archaic technicalities, too slow, too expensive and adversarial and that there was injustice when procedure received emphasis above the substantive issues of a conflict. He spoke of the “sporting theory of justice” where litigation was considered as a game where the lawyers were gladiators battling in court to win. He charged that the contentious procedure compels ‘counsel to forget that they are officers of the court and to deal with the rules of law and procedure exactly as the professional football coach with the rules of the court.’ At the time, Pound’s criticisms were considered scandalous, blasphemous and the ABA refused to publish the speech. Things changed however.
Thirty years later, Roscoe Pound went on to become Dean of the Harvard Law School and became a celebrated legal luminary. As for the legal system – Roscoe Pounds sentiments were not dismissed. Seventy years later in 1976, the then Chief Justice Warren Burger convened the Pound Conference (called the second Pound Conference, with the first attributed to Pounds’ 1906 speech event), to consider whether Pounds’ criticisms had been adequately addressed and what more needed to be done. Professor Frank Sander of the Harvard Law School delivered the keynote address and spoke of his vision for a comprehensive Justice center (the “multi door court house”) where an alternative system would function parallel to the litigation system and disputes would be directed to the most appropriate process, such as arbitration and mediation.
The impact of these discussions resulted in significant changes to the dispute resolution landscape in the USA through statutes, inclusion of ADR in academic courses, and the professionalization of the practice of ADR processes, including mediation. Currently, arbitration and mediation are recognized within the mainstream legal system with resounding success. All the States have recognized ADR pathways including mediation, in statutes. Mediation is well entrenched in the USA and the success rate is reportedly very high.
Australia has institutionalized mediation through several statutory and other initiatives. Courts are empowered to refer disputes to mediation without the consent of the parties to enable better management of civil matters. The Civil Dispute Resolution Act, 2011 contains provisions to ensure that, other than in respect of certain excluded civil proceedings, parties must take “genuine steps” to resolve disputes prior to litigation. The Act obligates parties instituting proceedings in court to file a “genuine steps statement” setting out the steps taken to resolve issues or the reasons why no such steps were taken and further provides that a Lawyer acting for such a party must advise that party of the requirement and assist that party to comply with that requirement.
In Ireland, in the very recent case of Burke v O’Connell [2026] IEHC 314 (May 20, 2026), the High Court considered whether a court can order parties to mediate a dispute, against their will, or whether a court is restricted to simply inviting the parties to mediate. Among other issues, the court considered whether mandatory court ordered mediation is a breach of a constitutional right of access to courts, and decided that a court delaying court proceedings for court ordered Mediation, even against the will of the parties, would not constitute a breach of the right access to the courts under the Constitution or the European Convention on Human Rights, and that judges in Ireland regularly make clear that the right of access to the courts is not unconditional. Importantly the court observed that the court is not directing the parties to reach an agreement but simply to commence a mediation. The Court also observed that a court directed mediation order is a very limited order which does not compel settlement and only requires parties to commence a Mediation process and that while attendance at Mediation may not be voluntary, reaching a settlement is voluntary and made order that a court, in controlling its own process, did have the power to direct Mediation in appropriate cases, and that it was an inherent power of the court to ensure the effective and efficient operation of the courts.
The Indian Mediation Act, 2023 articulates a pro mediation policy and provides for mediation via a court annexed scheme for which detailed statutory provisions are included. The Act states that parties may voluntarily, and whether there is a mediation agreement or not, take steps to pursue court annexed pre litigation mediation and provides for the steps to be taken therefor (section 5). The Act provides further that, even if such pre litigation mediation is unsuccessful, a court or tribunal may, at any stage of the proceedings, refer parties to undertake mediation and that when a court so refers a dispute, there is no obligation on the parties to come to a settlement (section 7). In respect of high value commercial disputes however, a plaintiff is required to exhaust ‘the remedy of pre institution mediation’ prior to instituting action, unless urgent interim relief is sought – section 12A introduced by the Commercial Courts, Commercial Division, and Commercial Appellate Division of High Courts (Amendment) Act, No. 28 of 2018.
In South Africa, parties are mandated to consider mediation before initiating litigation in the High Court. Challenged by a serious issue of a severe backlog, with trial dates scheduled even up to 2031, a Directive was issued by the Judge President of the Gauteng Division of the High Court along with a detailed process Protocol, effective April 2025 to require mandatorily that prospective litigants in all civil matters within the Gauteng division must participate meaningfully in a court-annexed mediation process before they can be allocated a trial date. The protocol requires, among other documents, that a Report of the Mediator stating, among other matters, whether parties “participated in good faith” be filed, to obtain a trial date. This requirement has been included to avoid what the Judge President refers to as “sham mediations.” (https://www.youtube.com/watch?v=v5Gmkzfu8gA&t=425s) Non-compliance results in matters being struck off the roll and could lead to adverse or punitive cost orders. Currently, a challenge to this Directive by the Personal Injury Plaintiff Lawyers Association and the Law Society of South Africa is pending, without a stay of the Rule.
Singapore has emerged as a global leader in the practice of mediation. The Mediation Act 2017 provides for a framework for the use of mediation and for enforcement of a mediated settlement agreement as a decree of court. Mediation is well entrenched in the legal system of Singapore and enjoys the support of government as well as the judiciary. Singapore played a key role in UNCITRAL in the deliberations that led to the drafting of the text for the 1998 UN Mediation Convention and was host to the Convention signing ceremony in August 1999 where a historical number of 46 countries, including Sri Lanka, signed the Convention on the very first day. Many of the training programmes for Sri Lankans that have been arranged by the International ADR Center, have been conducted by the Singapore International Mediation Centre (SIMC) which is renowned for its programmes and for services to handle international commercial disputes.
The European Union Directive (EU Directive 2008/52/EC) provides that a court may, when appropriate and having regard to all the circumstances of the case, invite parties to use mediation (Article 5.1) and that the Directive is without prejudice to national legislation to making the use of mediation compulsory or subjective to incentives or sanctions … provided that such legislation does not prevent the parties from exercising their right of access to the judicial system (Article 5.2). Many European countries have integrated mediation into their dispute resolution systems through legislation or procedural laws in ways that range from recognizing voluntary reference to mediation to requiring mandatory mediation for specified categories of disputes. Countries such as Italy, Greece, Germany and Belgium are some that have robust systems.
It is clear therefore, that jurisdictions around the world, irrespective of the legal system, have sought to recognize mediation for its value not only for minor community dispute resolution but also for the resolution of high value commercial and other family and civil dispute resolution. UNCITRALs preparation of the text for the 1988 UN Mediation Convention was inspired by the significant increase in the use of mediation in international trade and the need for a uniform regime for enforcement, such as the UN NY Arbitration Convention provides in respect of arbitration awards.
Sri Lanka’s advancements have thus far been driven by the private sector. A holistic approach to find responses to the backlog in courts to relieve the pressure on courts, is desired. The promotion of ADR, including mediation, deserves support from the government as well, since, clearly, laws delays have an adverse impact on the economy of the country and should not be seen only as an access to justice issue. As articulated in the UN Mediation Convention, among the positive beneficial results of using mediation for dispute resolution, is that there are cost savings for the State. It is a means of resolving disputes without detracting from the quality of the resolution.
by Dhara Wijayatilake
Attorney at Law; Former Secretary to the Ministry of Justice; Director and Secretary General of the International ADR Center

In recent years, falling trees have claimed lives, destroyed homes, and sparked an urgent debate: should Colombo’s ancient trees be cut down in the name of safety? But this is the wrong question. The real crisis is not that these trees are dangerous — it is that we have made them so. Through decades of road widening, root-smothering pavements, and indiscriminate branch cutting, we have steadily undermined the very trees we now fear. What we are witnessing is not nature failing us. It is us failing nature. As the world marks World Desertification Day on 17th June, Sri Lanka would do well to reflect that desertification does not begin only in distant, arid lands — it begins whenever a city turns its back on its own green heritage.
In recent years, falling trees have claimed lives, destroyed homes, and sparked an urgent debate: should Colombo’s ancient trees be cut down in the name of safety? But this is the wrong question. The real crisis is not that these trees are dangerous — it is that we have made them so. Through decades of road widening, root-smothering pavements, and indiscriminate branch cutting, we have steadily undermined the very trees we now fear. What we are witnessing is not nature failing us. It is us failing nature.
Colombo, our commercial capital, is considered one of the greenest cities in the world. This is highlighted by the award of the world’s first Wetland City designation to our administrative capital, Sri Jayewardenepura Kotte. Both cities and their green heritage should be treasured and protected — not only as assets of their citizens, but as a matter of national pride.
It is against this backdrop that one must view with deep concern the ongoing destruction of trees and greenery across Sri Lanka, particularly in urban settings such as Colombo and Kotte. The majestic trees lining our traditional tanks, rural areas, and urban areas are part of our heritage. The trees lining Colombo’s Ananda Coomaraswamy Mawatha (previously named the Green Path because of its large trees), Gregory’s Road, Thurstan Road, and Bauddhaloka Mawatha, are over a hundred years old. These are living monuments of our heritage. They provide shade, a natural canopy, and a habitat for a remarkable diversity of bird populations within the city. It is therefore vital that we make every effort to preserve these trees unless they pose a direct danger to human life.
Why Do These Trees Become Dangerous?
To address this question, we must first understand why large trees continue to fall during periods of strong winds. Old photographs indicate that it is we who have widened roads and built pavements to cover the roots of these majestic trees, a true heritage from the past.
A leading reason for trees to fall is age-related decay. Old trees tend to develop weak branches and trunks. Regular inspection of their structural integrity and timely treatment of disease would go a long way in preventing such failures.
The second reason is indiscriminate cutting of branches, which disrupts the natural balance of the tree. A principal offender in this regard is the Ceylon Electricity Board. When interviewing workers engaged in trimming city trees, one consistently hears the same justification: the branch must be cut because it is touching or close to a power line. There are no arborists, trained experts, or senior officials to guide these workers or determine whether a less destructive approach is possible.
The third reason is the destruction of root systems. Across the city, one can observe concrete and paving laid directly over the root zones of large trees. This prevents oxygenation and moisture from reaching the roots, causing them to deteriorate or die. The inevitable consequence is that the tree gradually loses its structural support at the base, making it vulnerable to falling.
What Should Municipalities and Town Councils Do?
To save our ancient trees, we must counter the flawed argument that we need to replace them—these trees are priceless “nature’s investments for hundreds of years” and, as a BBC article on ancient oaks suggests, their genetic heritage is vital for resilient future forests. See “1,000-year-old oaks used to create ‘super forest’ (See )
* A nationwide strategy is essential: we must start by strengthening the expertise of tree officers in the Colombo Municipal Council and other urban councils to ensure professional health assessments are available, while also linking with botanists, academics, and environmental groups at the University of Colombo.
* Use Google Maps and GIS for systematic mapping and reviving a citizen science platform, similar to one previously developed by University of Moratuwa, where students and the public can report environmental harm with photos and locations.
* Technology offers more powerful tools. There are Conventional Visual Tree Risk Assessment (VTRA) methods which fail to detect risks. More advanced methods were reported at the 30 th International Forestry and Environment Symposium 2026 e.g. Ground Penetrating Radar (GPR). These are able to find trunk decay and found examples in urban trees at Viharamahadevi park and Keppetipola road.
* We can raise public awareness through social media and community events like “tree walks,” a practice which could be further popularized by groups like Ruk Rakaganno (see ) and the Love A Tree Foundation (see )
* Finally, we must learn from international models like the UK’s Ancient Tree Forum (see ). The latter specialises in protecting trees as a heritage which must be preserved and protected for future generations.
by Saroj Jayasinghe
Emeritus Professor
Consultant Physician
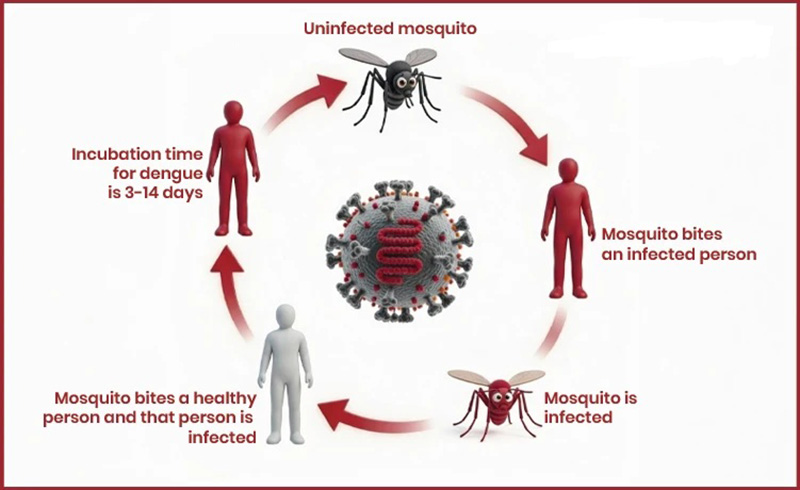
Dengue is one of the fastest spreading mosquito-borne viral diseases in the world today, posing a growing threat to nearly half of the global population. The World Health Organization describes dengue as a viral infection transmitted to humans through the bite of infected female mosquitoes, primarily Aedes aegypti and, to a lesser extent, Aedes albopictus. Once considered a disease limited to tropical regions, dengue has now expanded widely across continents, driven by urbanization, climate change, population movement, and weak vector control systems.
The global burden of dengue has increased dramatically over recent decades. According to WHO estimates, there are approximately 100 to 400 million infections annually, although a large proportion remain asymptomatic or undiagnosed. The disease is now endemic in over 100 countries, with Asia bearing the highest share of cases, followed by Latin America and Africa. As transmission intensifies and outbreaks become more frequent, dengue has emerged as a major public health concern requiring coordinated prevention and control strategies.
The nature of dengue infection
Dengue is caused by four closely related viruses known as serotypes: DENV-1, DENV-2, DENV-3, and DENV-4. Infection with one serotype provides lifelong immunity to that specific strain, but only partial and temporary protection against the others. This means a person can be infected up to four times in their lifetime.
Most dengue infections are asymptomatic or mild. When symptoms do occur, they typically appear 4 to 10 days after the bite of an infected mosquito. The clinical presentation includes high fever, severe headache, pain behind the eyes, muscle and joint pain, nausea, vomiting, rash, and fatigue. Because these symptoms resemble other viral infections, dengue is often underdiagnosed in early stages.
While most patients recover within one to two weeks, a small proportion develop severe dengue. This life-threatening condition is characterised by plasma leakage, severe bleeding, organ impairment, and shock. Without timely medical intervention, severe dengue can be fatal. WHO emphasises that early diagnosis and appropriate clinical management can reduce fatality rates to below 1 percent in well-managed settings.
Transmission and mosquito ecology
Dengue is transmitted primarily through the bite of infected female Aedes mosquitoes. These mosquitoes are highly adapted to urban environments and typically breed in artificial water containers found in and around homes. Unlike malaria-transmitting mosquitoes, Aedes mosquitoes bite during the daytime, with peak activity in the early morning and late afternoon.
The lifecycle of the mosquito plays a crucial role in transmission. Eggs can survive for months in dry conditions and hatch when they come into contact with water. Even small collections of water, such as flower pots, discarded containers, tyres, and water storage tanks, can serve as breeding sites.
Urbanisation has significantly contributed to the spread of dengue. Rapid population growth in cities often leads to overcrowding, poor waste management, and inadequate water storage practices, all of which create ideal breeding conditions for mosquitoes. Climate factors such as increased rainfall, humidity, and temperature further enhance mosquito survival and virus replication.
Risk factors and global expansion
Several factors increase the risk of dengue transmission. Population density is a key driver, as densely populated urban areas provide abundant human hosts for mosquitoes. Inadequate housing conditions and poor access to clean water force communities to store water in containers, which often become breeding grounds.
Human mobility also contributes to the spread of the disease, as infected individuals can introduce the virus into new regions where competent mosquito vectors are present. Climate change has expanded the geographical range of Aedes mosquitoes into previously unaffected areas, increasing the risk of outbreaks in both tropical and subtropical regions.
WHO has noted that dengue incidence has increased significantly over the past 50 years, with periodic outbreaks becoming more frequent and severe. The disease is now considered a major global health threat, comparable in burden to other high-impact infectious diseases in many regions.
Clinical management and absence of specific treatment
There is currently no specific antiviral treatment for dengue. Management is supportive and focuses on relieving symptoms and preventing complications. Paracetamol is recommended to reduce fever and pain, while non-steroidal anti-inflammatory drugs such as ibuprofen and aspirin are avoided due to their risk of increasing bleeding.
Patients with severe dengue require hospitalisation for close monitoring and supportive care, including intravenous fluid replacement and management of shock or bleeding. With proper medical care, mortality rates can be significantly reduced.
Early detection is critical. Warning signs such as persistent vomiting, severe abdominal pain, bleeding gums, rapid breathing, and sudden fatigue indicate progression to severe dengue and require immediate medical attention.
Prevention: the cornerstone of dengue control
Since there is no specific cure, prevention remains the most effective strategy against dengue. WHO strongly emphasises integrated vector management as the foundation of dengue control.
Personal protection measures are essential, especially during daytime hours when mosquitoes are most active. These include the use of mosquito repellents containing DEET, picaridin, or IR3535, wearing long-sleeved clothing, and using mosquito nets when resting during the day. Window and door screens also help reduce indoor mosquito exposure.
Environmental management is equally important. Communities are encouraged to eliminate breeding sites by removing stagnant water, disposing of waste properly, and cleaning water storage containers regularly. Even small water collections can sustain mosquito populations, making household-level participation crucial.
Public health programmes also rely on insecticide spraying during outbreaks to rapidly reduce mosquito populations. However, WHO emphasises that chemical control alone is insufficient without sustained community involvement and environmental management.
Community participation and public health response
Community engagement is a central pillar of dengue prevention. Effective control requires continuous participation from households, schools, workplaces, and local authorities. Public awareness campaigns play a vital role in educating populations about mosquito breeding habits and personal protection measures.
Surveillance systems are also essential for early outbreak detection and response. Health authorities monitor dengue cases and mosquito populations to identify high-risk areas and implement targeted interventions.
Integrated approaches that combine environmental management, biological control, chemical interventions, and public education have proven most effective in reducing transmission.
Vaccination and emerging tools
In recent years, dengue vaccines have been developed and introduced in some countries under specific conditions. WHO has recommended the use of certain vaccines in areas with high transmission, particularly for populations with prior exposure to dengue. However, vaccination strategies remain limited and must be carefully implemented due to the complexity of immune responses to dengue infection.
Research continues into new tools such as genetically modified mosquitoes, Wolbachia-infected mosquitoes that reduce virus transmission, and improved diagnostic technologies. These innovations offer promising additional tools but are not yet substitutes for established prevention measures.
Dengue remains a rapidly growing global health challenge with significant medical, social, and economic impacts. Its spread is driven by urbanisation, climate change, and the adaptability of mosquito vectors. While no specific cure exists, timely clinical care can prevent deaths, and effective prevention strategies can significantly reduce transmission.
The World Health Organization emphasises that dengue control depends on a combination of personal protection, environmental management, community participation, and strong public health systems. As the disease continues to expand geographically, sustained global commitment is essential to reduce its burden and protect vulnerable populations.

Hundreds of cats stolen for food in Vietnam rescued by police, welfare group says

Canada-Netherlands ODI abandoned due to dangerous pitch in Toronto

Da Silva and Jangoo earn recalls for West Indies’ Tests against Sri Lanka

Spinners make it two in two for England

Messi hat-trick fires holders Argentina to win over Algeria at World Cup

UNDP, Central Bank deepen financial literacy drive to build economic resilience

‘Dates have the highest sugar content to fight Coronavirus’

Sunday Island 27 December – Headlines

#SundayIsland 17th December – Headlines

Sunday Island – 28th March

Sunday Island Headlines – 21 March

Sunday Island – 21st February – Headlines
-

 News5 days ago
News5 days agoCIABOC summons Yoshitha over his participation in British Navy training programme
-

 Sports2 days ago
Sports2 days agoTharanga set for high-profile javelin clash in Ostrava
-

 News5 days ago
News5 days agoJustice Minister responds to social media claims he represented Easter Sunday ringleader
-

 Features3 days ago
Features3 days agoPolitics of protected species
-

 News4 days ago
News4 days agoCommonwealth lawyers urge Lanka to uphold rule of law
-

 News2 days ago
News2 days agoRelease of 2025 O/L results likely to be delayed
-

 News2 days ago
News2 days agoTheft of USD 2.5 mn from Treasury: CoPF accused of complicity in NPP cover-up
-

 News1 day ago
News1 day agoBeijing Capital Airlines to resume flights to Colombo signalling boost to tourism