Features
COVID 19 containment – the role of Mass Media in changing peoples’ behaviour

by Lakshman Wickramasinghe
Sri Lanka is entering the riskiest period in its battle against Covid-19, with the British Covid 19 variant now accepted as responsible for rapid escalation of infection rates and the danger of the Indian variant coming ashore through illicit landings. At this stage the most effective response to the virus is the sustenance of behaviour changes already adopted by the majority of the population, and the promotion of right behaviour among the laggards.
The health sector which is responsible for developing technically appropriate messages for changing behaviour of people has been doing magnificently in formulating such messages. The Health Education Bureau renamed the Health Promotion Bureau did a splendid job in planning and broadcasting TV spots in association with many mass media channels as Covid-19 appeared in Sri Lanka. It was a commendable behaviour change communication initiative made with a low budget but with high creativity with a lady doctor being the main communicator.
I was wondering why such an initiative had not yet started by the Health Promotion Division in response to the New Year infection cluster but was happy to note that a few days ago two new TV spots have been launched through the State TV channels. Rupavahini also started a novel TV spot showing Covid 19 viruses conspiring to invade places where big crowds congregate. With Covid infections assuming dangerous proportions, the Sri Lankan mass media too has a responsibility to increase its support to Covid-19 behaviour change communication activities.
However, health communication initiatives launched against Covid-19 unfortunately has had to face constraints globally. This is why Dr. Tedros Adhanon Ghebreyesus, the Director General of WHO, was perhaps constrained to declare at the Munich Security Conference on February 15, 2020 that ‘we are just not fighting an epidemic, we are fighting an infodemic’ as reported in the Lancet.
This internationally acclaimed medical journal in its editorial (Vol.395, Issue10224, pg.537) of February 22, 2020 commented: “The ease through which inaccuracies and conspiracies can be repeated and perpetuated via social media and conventional outlets put public health at a constant disadvantage’.
The question to be asked then is should the government health sector, the prime defender against epidemics, be put under ‘a constant disadvantage’ by newly arrived digital media and the conventional mass media, and players connected to power politics. The answer is No.
No country can expect much support from social media in this regard. This is especially so in a country that is multi-cultural, multi-religious and with the presence of a large number of fringe political entities, folk beliefs, superstitions etc. It was only yesterday that the Ministry of Ayurvedic Medicine had to issue a press communique requesting the general public not to use various ‘prescriptions’ of local medicines published in the internet and social media.
Thus it is the main stream mass media (i.e. print, radio, and television) that has the prime responsibility for helping to creating a positive environment for the adoption of recommended behaviour by the public. Despite the cacophony of big and small alternate media, the mainstream media channels are still accepted by the vast majority of Lankans as channels that inform, educate, and entertain. They still enjoy high credibility.
In this respect it is appropriate to examine how mass media could support the government health sector. First and foremost the mainstream mass media should formulate programmes founded on authentic communication principles to genuinely and without any other agendas persuade their readers, listeners and viewers, to behave as recommended by government health authorities.
Trust and credibility of the message and its sender (or the source) is central to this objective. The clarity of message especially with regard to ‘what’ and ‘how to’ behave in the context of the current challenge and the benefits of adoption is also important. The ‘conveying of a sense of unity of messages’ is also vital. The other critical factor is the reduction of what is known as “noise” in communication jargon. This ‘principle’ prevents the main message getting lost among related but discordant messages. In this regard Rupavavhini has done well during the last two to three weeks through its morning discussion programmes.
The media (through all their programmes and features) should help to build trust among the citizenry on the ‘package of key health messages’ disseminated by the health authorities and the government. Trust is key to acceptance of behaviour change messages. So is the credibility of the source of information (the state health authority and the government in this case). They should simultaneously be promoted. These two go hand in hand as one reinforces the other. The primacy of promoting trust and credibility of the messages and the source should be a universal standard cutting across all else. Even if two or three programmes broadcast by a channel create a negative perception in their audiences then the attempts of the rest of the programmes to promote trust and credibility will be devalued.
Therefore in emergency situations such as in combating pandemics, the media through all of its major editorially driven components should support instilling of deep trust in the primacy of the messages and the credibility of the source. This ‘conveying of a sense of unity’ across all of its programmes is a must for promoting high behaviour change rates.
For example a TV channel in a ‘Meet the Doctor’ programme shown during non- prime viewing time would advise its audience to desist from going on picnics or pleasure trips during this critical period. Few hours later a popular teledrama episode aired at peak times would show the hero and heroine going on a fun-filled picnic with three four other friends to a popular crowded picnic spot. Such a programming mix would be most harmful as what is important is to drive home the message “don’t go on picnics at this time.” If this is unavoidable as the episode has been filmed before the New Year cluster appeared, then an appropriate explanatory line below the particular picnic shot can support unity of the key message.
Another example is that different TV stations would subtly promote particular political parties or ideologies and I believe that in a democracy this is acceptable. But in a national emergency such as Covid-19, the presentation of key behaviour change messages close to news or features relating to criticism of government programme on Covid 19 management would not convey a sense of unity of the messages. (Of course this may be debatable.) Further, such a mix would also negatively affect the trust of the audience in the key Covid 19 protection message and may also to some extent affect the credibility of the source. This is no easy question to resolve and would be akin to ‘walking on a tight rope’. But these are possible practical examples and the communication programmers must reflect deeply on striking a balanced approach where the national responsibility of promoting behaviour change is sustained while presenting investigative journalism productions.
One way of overcoming these obstacles is for all or most mass media channels to run an identical behaviour change communication campaign so that the key messages in regard to Covid 19 would be promoted by all key channels, thus displaying the concept of unity of messages. An initiative such as this would convey to the general public that irrespective of individual policies, and political sympathies, all media channels are interested in a national campaign to promote behaviour change, thus exponentially enhancing behaviour change persuasion.
Such a media campaign could be developed by one or a group of advertising agencies as their contribution to the national cause in coordination with the Ministry of Health and the media channels can broadcast programmed TV spots free of charge as their own contribution to a national cause. A prime example of such a campaign was the ‘Api Wenuwen Api’ campaign run during Eelam War IV. Currently, if such a common campaign is envisaged rapidity of implementation is critical for controlling the epidemic.
(The writer is a retired Officer of the International Civil Service of the United Nations system attached to UNICEF and a Behaviour Change Communication Practitioner. He also worked as a UNFPA consultant at the Health Education Bureau.)
“We are rather respectable in Colombo. We go to bed fairly early, and we remain there till morning. “
According to Sri Lanka’s diplomatic folklore, the late S.W. R. D. Bandaranaike uttered these words while explaining the reasons for Sri Lanka’s abstention on the UN resolution condemning the Soviet invasion of Hungary. Apparently, SWRD’s foreign ministry officials were asleep at home when the diplomatic cable seeking instructions was received from New York. In those days, there were no cell phones, Internet, or even fax or telex machines. The diplomatic cables were sent through post offices. Decoding them was a slow and time-consuming process. Thus, the government could not provide appropriate instructions to our mission in New York in time, and the Sri Lankan delegation abstained on that sensitive UN vote.
Sri Lanka’s Absence from Section 301 Consultations
But then, how does one explain Sri Lanka’s absence from the crucial bilateral consultation held in Washington by the Office of the United States Trade Representative (USTR) during March-April on “Forced Labour” under the Section 301 of the US Trade Act of 1974? Didn’t our foreign and trade ministries send appropriate instructions to Washington in time? Even if the instructions from the foreign ministry were transmitted to our embassy in Washington by pigeon carriers, there was enough time for Sri Lanka to participate in those meetings.
In March, the USTR initiated these 301 investigations on 60 trading partners, and invited all of them for confidential consultations. Out of the 60, 46 participated in these consultations. Sri Lanka was not one of them. Other countries that didn’t participate in these consultations included China, Russia, and Venezuela! In addition to that, the Section 301 Committee conducted a public hearing with interested parties on April 28 and 29. Washington-based diplomats, representatives from few trade ministries as well as representatives from many foreign trade associations and chambers participated in these hearings. Sri Lanka was once again conspicuously absent.
As a result, when the USTR published the proposed forced labour tariffs on June 2nd, Sri Lanka ended up with a 12.5% duty. Pakistani and Indonesian diplomats participated in these consultations and took appropriate follow-up measures, and managed to enter the 10% duty category. As even a threat of a modest tariff hike could disrupt supply chains and reduce competitiveness, particularly in an industry such as garments, I discussed this issue on 15 June and underscored the importance of Sri Lanka’s participation at the next hearing, which was scheduled to be held from July 7th .
Awakening from Diplomatic Slumber and AKD’s Gazette
Fortunately, Sri Lanka finally awoke from weeks of diplomatic slumber, and Ambassador Mahinda Samarasinghe participated in the public hearing on 9 July, and promised, “…. · We have agreed to the text in our negotiations with the USTR on forced labour, …. The gazette as we speak is being printed and I’m getting the gazette tomorrow morning, and the gazette will be shared with USTR as I get it“.
As promised, President Anura Kumara Dissanayake issued a gazette on 10 July banning the imports of goods produced by forced labour. These new regulations are very similar to what Pakistan and Indonesia enacted in April, after their consultations with USTR in March. Why couldn’t we do it in April? Why did we wait till the very last minute?
Challenges ahead
“War is too important to be left to generals alone,” is a famous saying attributed to former French Premier Georges Clemenceau. Similarly, monitoring our main markets is too important to be left to diplomats alone. The United States is the largest single-country market for Sri Lanka. Therefore, Sri Lankan trade chambers and associations should become more proactive in these markets and participate in these events. For example, the chairman of the Pakistani apparel exporters association participated in the April hearings. Similarly, representatives from the Indian Agricultural and Processed Food Products Export Development Authority, the Federation of Indian Chambers of Commerce and Industry, the Confederation of Indian Industry, and Reliance Industries also participated in July hearings. At an event where each speaker is given only five minutes (strictly enforced), having a number of speakers from a country is an advantage. The presence of industry representatives in these kinds of events also help them understand the market dynamics and the future challenges. This is important, particularly because there will be many more challenges with Trump’s tariffs.
With the gazette issued on 10 July, Sri Lanka has imposed a prohibition on the importation of goods produced with forced labour. Now, the challenge will be to effectively enforce the prohibition. And what are the goods produced with forced labour? The USTR list only focuses on aluminum, cotton, electronics, lithium-ion batteries, rice, and tobacco. However, according to the U.S. Department of Labour, the list is much longer. Hence, this list may change continuously during the next two years and tariffs may fluctuate once again.
So, this is definitely not the time to slumber.
(The writer, a retired public servant, can be reached at senadhiragomi@gmail.com)
by Gomi Senadhira ✍️
After the overwhelming grotesquerie of J K Rowling’s latest Cormoran Strike novel (written, I should have noted, as the others were, under the pseudonym Robert Galbraith), I thought I should return to the world of fun, and also a much shorter description since this thriller moves quickly without the layers of detail that Rowling engages in.
I then move to the second comic thriller by Caryl Brahms and S J Simon. This, their second story to feature Vladimir Stroganoff and Adam Quill, was Casino for Sale, as lunatic a romp as the first, though without the emphasis on the ballet that characterized A Bullet in the Ballet.
This one begins with the impresario Stroganoff buying a casino cheap from Baron Sam de Rabinovich, only to find that it was a rundown place, not the grand casino of La Bazouche, a resort on the Frenc+h Riviera, as he had initially thought. The grand one belonged to Lord Buttonhooke, and Stroganoff could not compete, until he thought of bringing the Ballet Stroganoff to the casino – which of course leads to Buttonhooke deciding to have ballet performances in his Casino too.
Stroganoff invites Quill to visit him, which Quill decides to do since he has left Scotland Yard, having come into a legacy. No one believes this, and he has to face questions as to what he did to have been sacked, with sympathy for having been found out.

Caryl and Simon
The day he arrives in La Bazouche there is a murder, of a vitriolic critic called Citrolo, in Stroganoff’s office. He had been going to write a damning review of the opening night of the ballet and Stroganoff, when he realizes Citrolo cannot be swayed, drugs him and dictates the review himself to the papers. He leaves Citrolo sleeping and finds him shot the next morning, whereupon he decides to muddy the waters and leave a suicide note and lots of other murder weapons. So much overkill, as it were, of course ensures that he is arrested.
But the excitable French detective who makes the arrest follows up his suggestion that Buttonhooke was also involved, and so the two casino owners find themselves in cells next door to each other, with the detective Gustave quite happy to provide creature comforts for a fee.
Quill decides he must investigate, and finds Gustave most cooperative, since he has a laid back attitude to work. So it is Quill that finds a notebook which makes it clear Citrolo is an accomplished blackmailer, and that there are lots of possible murderers, including Stroganoff’s croupier, who was crooked, Rabinovich, who was now working for Buttonhooke, a confidence trickster called Kurt Kukumber, whose prospectus for a dud gold mine was found in the office and Prince Alexis Artishok who was engaged in a deal to buy diamonds from the ballerina Dyra Dyrakova.
Stroganoff had been trying to get Dyrakova to dance for him, but having done so previously she had refused. But then to Stroganoff’s chagrin she agreed to dance for Buttonhooke. The clearly crooked Artishok had told Buttonhooke’s mistress Sadie Souse, who was not very bright, that Dyrakova possessed diamonds she was willing to sell cheap, and Sadie was determined to have them.
Quill meanwhile finds out that there was a secret passage to Stroganoff’s office, the obvious solution to what had begun as a locked room mystery, and that this was known by almost everyone apart from Stroganoff himself. And then Rabinovich is murdered, just after Gustave had released his two original suspects, leading him to blame Quill for having insisted on that and thus allowing them to kill again.
Soon afterwards Dyrakova arrives, and the town is full of posters announcing that she will appear in the casinos, elaborate posters for either one, since Stroganoff is determined that she will dance for him, and if she does not come willingly, he has devised a scheme to make her do so unwillingly. So, though Buttonhooke has her taken off to his yacht immediately she arrives at the station, Quill along with Arenskaya gets her into a launch and to Stroganoff’s casino, where she performs to tumultuous applause, not knowing for whom she is dancing.
When Quill asked her about the diamonds, she said she had sold them long ago, and that gave Quill the solution to the mystery. Rabinovich had known about this, and Artishok had killed him to prevent Sadie learning it from him, he had killed Citrolo who had recognized him for an accomplished card sharper, not a Russian prince at all. But before he is arrested, he gets away in a boat, and the police launch that pursues him is on the point of catching him up when it runs out of petrol.
Again, lots of excitement, and entertaining references – Gustave grows marrows – and if not quite as brilliant as its predecessor, Casino was certainly a delightful read.

 It was a few years back that a former President of Sri Lanka took it on himself to pronounce SAARC ‘dead’. Since then there have been other sections of Sri Lankan opinion that have joined the critics of SAARC and taken the solemn stance that SAARC has indeed died what may be called a natural death.
It was a few years back that a former President of Sri Lanka took it on himself to pronounce SAARC ‘dead’. Since then there have been other sections of Sri Lankan opinion that have joined the critics of SAARC and taken the solemn stance that SAARC has indeed died what may be called a natural death.
Their fatalism is understandable. SAARC has failed to meet at heads of government or state level for the past several years to take the SAARC process notably forward. Regional cooperation has more or less been only an appealing idea. No substantive concrete projects have taken off to make the idea a hard reality. ‘Inner paralysis’ seems to be SAARC’s lot. Hence the fatalism in these circles.
However, being one of the worst cash-strapped regions of the world and a teemingly populated one with people virtually left to their devices, what choices do the ‘SAARC Eight’ have other than to try their best to band together and continue with their cooperation efforts, however small they may be?
There is no escaping the mounting debt trap for many of these countries and bankrupt Sri Lanka is a glaring example, but ‘throwing in the towel’ and abandoning themselves entirely to the diktats of the strongest economies and their agencies will prove a ‘living death’ for many countries in the SAARC fold.
The gains may be meagre but giving-up on SAARC cooperation in full would prove self-defeating for the organization and South Asia. Right now, the collective intention ought to be to salvage what the region could from the tenuous cooperative efforts. Moreover, such initiatives could go some distance to generate a degree of goodwill among the Eight and help in sustaining a dialogue process.
Given this backdrop it proved ‘a stich in time’ for the Regional Centre for Strategic Studies (RCSS), Colombo, to recently host the SAARC Secretary General Ambassador Md. Golam Sarwar to a round table discussion on the unifying potential of SAARC and its future possibilities, besides other related issue areas.
Held on June 24th and moderated by RCSS Executive Director and former ambassador Ravinatha Aryasinha, the forum brought together a vibrant, wide ranging audience comprising academicians, diplomats, senior public servants, civil society activists and many others. Following the presentation by Ambassador Golam Sarwar titled, ‘Reigniting SAARC: Achievements, Challenges and the Way Ahead’, a lively Q&A followed.
The above forum could be described as an act of lighting the proverbial ‘candle’ rather than ‘cursing the darkness.’ It surely is a ‘darkness’ that could be seen as daunting considering that the region’s pivotal powers, India and Pakistan, are failing to act in a spirit of accord but are engaged in bitter finger-pointing on a number of questions of vital importance to SAARC.
On the other hand, what is the rest of the region doing to bring the above sides together? It is disappointing that to date the rest of SAARC has failed to launch a major diplomatic drive to bring peace between the feuding regional heavyweights. It needs to act without delay and establish its earnestness and this effort would need to prove SAARC’s staying power in the unfolding months and even years.
In assessing SAARC’s seeming failure local opinion in particular has failed to factor in what could be described as weak leadership. Since Sheikh Mujibur Rahman of Bangladesh, the founding father of SAARC, the region has failed to produce a visionary leader who could advance the SAARC cause with charisma and drive.
Among other reasons, weak leadership accounts considerably for the faltering and stuttering status, as it were, of SAARC. Badly needed are leaders who could go the extra mile, think less of narrow national interests and work diligently towards the collective well being of the region but SAARC’s millions of ordinary people have been made to wait in vain for leaders of such stature. Instead, they have been burdened with politicians who seem to be relishing the apparently moribund state of SAARC.
Looking back, it could be said that it was the dynamic leadership factor that led to the launching of the Non-Aligned Movement and for its sustenance for a few decades. True, it could be seen in some quarters that NAM is no more, but as in the case of SAARC, the former too has been unfortunate to be burdened over the years with politicians who lack the vision and drive to unflaggingly advance the fortunes of the South. NAM and SAARC lack the dynamism and vision of leaders of the stature of Jawaharlal Nehru, for example, to give them the required guidance and intellectual depth.
The reasons are complex for there not being among us currently political leaders with the vision and the steadfast commitment to advance the legitimate interests of the South. However, it could be stated with conviction that the majority of Southern leaders have too easily caved in to the demands of the global North and its financial agencies.
These leaders have failed to see, for instance, that the largely market economy oriented Northern governments would not view with favour a centrist economic model that attaches priority to the interests of the dis-empowered publics of the South. This realization ought to have dawned on the current government in Sri Lanka, for instance, some while ago but it has no choice but to abide by IMF dictates since economic survival at present is unthinkable without the latter’s succour.
Accordingly for SAARC this should be the time for some soul-searching. Priority needs to be attached to ending the feuding between India and Pakistan since at present the material fortunes of the region hinge largely on these regional giants giving peaceful relations among them a try. This is no easy challenge to meet but some daring, visionary diplomacy needs to take hold among the rest of SAARC.
There is some sense in SAARC bringing the peoples of the region together through programs that address their best collective interests. A meeting of minds among SAARC nations could enable SAARC and its agencies to build a region-wide people’s movement for progressive political and economic change that could in turn lead to the region’s political leaders sensitizing themselves more to the neglected needs of their publics.
However, the time is ‘now’ for the initiation of these progressive changes and the voice of SAARC well wishers would need to drown out those of their critics.

Davis cup Asia/Oceania Group IV 2026 to be held in Colombo from 20th to 25th July

Navy brings fisherman in distress off Pothuvil, ashore

Malinga, Asalanka seal Galle Gallants win in LPL opener

Showers may occur in the Western, Sabaragamuwa and North-western provinces and in Kandy, Nuwara-Eliya, Galle and Matara districts

Dengue outbreak gallops ahead: Infections surpasses 73,455, leaving 50 dead

Evidence recorded in money laundering case against Yoshitha Rajapaksa

‘Dates have the highest sugar content to fight Coronavirus’

Sunday Island 27 December – Headlines

#SundayIsland 17th December – Headlines

Sunday Island – 28th March

Sunday Island Headlines – 21 March

Sunday Island – 21st February – Headlines
-

 Features6 days ago
Features6 days agoPrison riots and politics: NPP’s biggest challenge and Sri Lanka’s biggest opportunity
-
 Features3 days ago
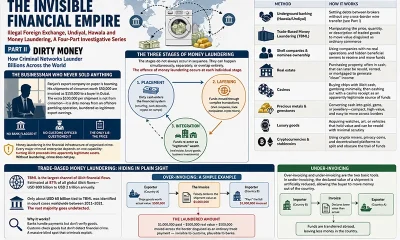
Features3 days agoDirty Money
-

 Editorial6 days ago
Editorial6 days agoMuch ado about crime: Fish or cut bait
-

 Features6 days ago
Features6 days agoMore on Saudi Arabia: ARAMCO and beyond
-
 Sports6 days ago
Sports6 days agoThe banker who rescued Sri Lankan cricket
-

 News1 day ago
News1 day agoMoney laundering case against Yoshitha, fixed for pre-trial conference
-

 Midweek Review3 days ago
Midweek Review3 days agoThe sordid tale of theft and tragedy at Finance Ministry
-

 Latest News4 days ago
Latest News4 days agoOil prices hit 1-month high as US-Iran attacks dim Strait of Hormuz outlook