Features
The agony and the ecstasy of the drink of the Gods

By Dr Nihal D Amerasekera
“In beer there is freedom,
in wine there is health,
in cognac there is power,
and in water there is bacteria.”
—Anonymous
Fermented beverages have existed since the neolithic period 10,000 BC. Alcohol has played an influential role in many ancient cultures and civilisations from China to Egypt. Romans even had a God of wine, Lord Bacchus. The Greeks had Dionysus, God of wine and ecstasy.
Many of us are social drinkers. Alcohol is a drink that reaches the parts of the mind to mesmerize, captivate and enthral us. The amber nectar can reduce inhibitions and make social interactions easier. At the opposite end of the spectrum alcohol has the propensity to create mayhem, destroy families and ruin lives. It is almost impossible to predict if a person will remain a social drinker or turn into an alcoholic. This uncertainty together with the sinister dark side of drinking there are strong enough reasons to remain teetotal. Many of the religions forbid the consumption of alcohol. There are many in the world who abstain and sip nothing stronger than aqua-minerale.
I’ve been a drinker for much of my life. I remember with such clarity my very first drink. It was Christmas and I was an inquisitive 14-years old spending a holiday with my cousins in a rubber estate in Warakapola. The grownups were merrymaking and the booze flowed freely. They all had a late night and were in a deep slumber. My cousins and I raided the drinks cabinet. We drank far too much than was good for us and were sick as parrots. It was a lesson learnt the hard way to regulate and pace our drinks.
The drinking culture is well established at universities. There is a tendency to feel excluded if one doesn’t drink. As a fresher there is much peer pressure to drink and also to drink in excess. It is a perfect breeding ground for alcohol addiction. As I joined the medical faculty drinking started with the rag and continued into the infamous Law-Medical cricket match. During the match booze was dispensed from barrels, an excuse to drink in excess and misbehave.
This was more youthful exuberance than hysterical nonsense. This culture somehow drifted seamlessly into the final year. There were many boozy evening parties held at the faculty’s Men’s Common Room. This was our paradise where we felt liberated. It was tremendous fun. My abiding memory of those parties is the music and the dancing in various stages of inebriation. I never missed an opportunity to join in the fun. They will always remain a wonderful memory of the happy and carefree days of my youth. I admire and applaud the few who had the courage of their convictions to remain sober and still enjoy the fun and the frolic of those parties. Some held a glass of ginger ale to create an optical illusion.
My father enjoyed a drink but I have never seen him drunk. While I was at University, he sometimes offered me a drink. But I was too shy and too respectful to drink with him. After I qualified as a doctor, we enjoyed a tipple together. He always poured his own and allowed me to do the same. Father seemed to love this ritual. I think it gave him immense pleasure.
The early 1970’s wasn’t a particularly happy time in my life. I was working at the Central Blood Bank in Colombo. I pined for friendship to forget my troubles. I became a pillar of the Health Department Sports Club at Castle Street. The Club was a magnet for health workers who loved a drink and a chat in the evenings. There I was never short of company. I can still remember the bar, the ambient lighting and the soft canned music that played continuously.
We talked politics, philosophy and careers and a multitude of other fascinating subjects that were made compelling by the amber nectar. Cheap and cheerful, arrack was our drink, it seemed to soothed my pain. On an evening It gave me immense pleasure to walk through those familiar portals of the Club. A day that stands out in my memory is when a few had gathered around the smoke-filled bar. On that warm evening I sat with my drink over-looking the shimmering lights of the surrounding buildings.
As the night wore on a young lad strummed his guitar and began to sing those well loved popular songs of CT Fernando, Chitra and Somapala and Sunil Santha. I remember well his beautiful rendition of that all time favourite “Tika venda nala, konde kadala”. The cleverly parodied sensuous lyrics were an instant hit. As I walked to my car that evening I could still hear the clapping and the slurred voices in the distance.
At times, I realised to my horror, I was there at the Health Department Sports Club for a drink all on my own. This wasn’t a good sign. Living with my parents I was never short of sound advice although much of it went unheeded. It is easy for alcoholism to take hold insidiously. What hounded and heckled me often was a short verse in our pharmacology textbook by D.R Laurence. In his brilliant description of the treatment of alcoholism was the sombre lament of an alcoholic who had accepted the inevitable “Doctor, goodbye, my sails unfurled I’m off to try the other world”.
My life then was on a spiral of decline. What finally saved me from seeing pink elephants was the constant nagging of my parents and the news of the MRCP(UK) Part 1 examination to be held in Colombo for the first time. The latter gave me an opportunity to focus on a worthwhile ambitious project. I had to buckle down to some hard work and also to move away from the tight grip drink had on me.
Giving up the carefree life I loved was a colossal task. Good friends and friendships are worth their weight in gold. The energy, enthusiasm and the sheer determination of my ambitious friends at the General Hospital Colombo steered me in the right direction. As I burnt the midnight oil, crystal clear Labugama water became my favourite drink. Success at the examination was a defining moment in my life. I had finally left my troubles behind and celebrated with friends, where else but at my beloved Health Department Sports Club. Not many have the good fortune to return from the brink as I have done.
Moving to work in England required a work ethic and self-discipline. The onerous routines of ward work and on-call duties kept me busy and fully occupied. I had to remain sober to study and appear for professional examinations. Then came marriage and a young family requiring self-restraint. During those years alcohol was a rare luxury. As the children became teenagers nearing 18, we enjoyed a drink together as a family. Drinking then was confined to wine although my preferred drink was whisky. Watching cricket has always been my passion. I have such fond memories of the exhilarating effects of Champagne watching cricket at the Lord’s cricket grounds, bathed in the summer sunshine.
Reflecting on my years in hospital, I recall the busy hustle and bustle of patient care. The hospital is also a place of friendship and camaraderie. The doctors often gathered together for joyful soirees, formal dinners and posh parties. At those events no expense was spared. The drinks flowed freely, they were lively, entertaining and most memorable. By then drinking and driving had become a serious crime. We all have learnt to drink sensibly. Those who let their hair down and drank a few more for the road, were taken home in taxis.
Retirement left time on my hands. There is now a great desire to have a drink in the evenings to help while away the time. Alcohol does give an extra boost when watching sports or a film or listening to music. I have found to my disgust that I cannot now tolerate alcohol as much as I did in my youth. The hangovers are more unpleasant and tend to last longer. Despite all that I still enjoy a drink. For my age I need to take greater care to protect my health. I have learnt to enjoy and appreciate the seraphic peace of sobriety during the week, enjoy wine at weekends and whisky only on special occasions.
The drinks industry worldwide is huge and they support a well-established drinking culture. With drinking so widespread it is important that we are all aware of its hazards. Education is key and is a long term commitment to make us all mindful of the risks and benefits of drinking. This should be done in schools and universities. Religious leaders can play an important role too.
There has been much publicity in the medical literature about the calamitous consequences of drinking. The safe limits are quantified in units. I take a cue from the experts for advice and would recommend visiting the website Much more can be done by the media to bring this issue out into the open. I have often wondered, if I knew as a teenager, what I know now about alcohol, whether I would be a teetotaller today.
Life is tougher now than in my youth and certainly more competitive. Navigating through life can be daunting and even traumatic. Through my own experience I realise how easy it is to depend on alcohol as a helpful prop. I know for certain that in reality, alcohol can never shield me from life’s problems. Drink can so easily spiral out of control and drift into the path of no return.
I remember with much nostalgia and great sadness the many school friends and medics who died of alcohol related illnesses. My best friend, who rose up to become the head of the Cancer Institute at Maharagama sadly succumbed at the age of 58. He was talented and had much to offer society when he was sadly snatched away. May this brief narrative be a dedication to his memory. May his Soul Rest in Peace.
Features
‘There are no private universities in Sri Lanka’ – some considerations for higher education reform

 Academics involved in education policy like to say that there is no such thing as a private university in Sri Lanka. The only ‘universities’ in the country are state universities; anything else offering degrees is a private higher education institution (HEI). This position is technically accurate. Yet, in the discourse and imagination of the public, private universities are very real – people teach in them, students register in them, families pay fees, and such degree holders enter job markets in Sri Lanka and outside.
Academics involved in education policy like to say that there is no such thing as a private university in Sri Lanka. The only ‘universities’ in the country are state universities; anything else offering degrees is a private higher education institution (HEI). This position is technically accurate. Yet, in the discourse and imagination of the public, private universities are very real – people teach in them, students register in them, families pay fees, and such degree holders enter job markets in Sri Lanka and outside.
For decades, activists concerned for public higher education have ignored or resisted looking at private HEIs, as if such scrutiny would taint them. Others have worked in both types of institutions, carrying practices from each to the other. The apex body governing state universities, the UGC, has, meanwhile, ignored the concept of conflict of interest and appointed individuals in private higher education in committees and leadership positions. It is unsurprising then that some of the ideologies informing private higher education appear in reform agendas in the state sector.
This is a good time then to consider the varying types of private HEIs around us, and to take a look at some of the issues within them in the hope that higher education reform agendas will include private, as well as state higher education.
What is a ‘private university’?
First, some clarifications. In the public imaginary, a ‘private university’ is typically an institution that provides a foreign or local degree for which the student makes a payment. But this broad classification encompasses a host of diverse institutions and types of degrees which I detail below.
The Non-State Higher Education Division (NSHE) of the Ministry of Education has recognised 295 degrees by 32 institutions. Most of these are private companies and include a handful of established, well-known private HEIs that are ‘university like’. The degrees are local degrees conferred by the institutions accredited by the NSHE Division. While private HEIs conferring local degrees must be accredited by the NSHE Division, there appears to be no legal consequence for not doing so. In addition, there are several permutations of the private degree that miss the net of this Division and the Standing Committee on Accreditation and Quality Assurance (SCAQA) that assists this Division.
For one, degrees conferred by foreign universities offered, via these same private HEIs, are not vetted by the NSHE Division. Secondly, there is a growing plethora of private HEIs which have either no physical presence locally or only a dubious presence. The University Grants Commission has notified the public, through their website, that foreign universities listed in the Commonwealth Universities Yearbook and the World Higher Education Database are recognised, but refrained from giving any other details – which degrees? Offered by what modes? These details are not known. Some of the foreign universities in the lists may be legitimate entities in their own land but the degrees conferred locally, in their name, may not adhere to curriculum or teaching specifications of the NSHE Division or the UGC.
Another troubling phenomenon is the ‘top up degree’, which appears to work on the same principle as that of a pre-paid mobile connection: if I have a Diploma or an HND of a sort, I am eligible to complete a course of study which provides me with a degree, usually from a foreign university. The idea that someone who does not initially qualify for a degree programme should be able to work their way towards one is a progressive notion. This is the concept that open and distance learning (ODL) was based on initially, but which is now sadly exploited. ODL models are expected to provide opportunity for learning for those who may be excluded from traditional learning institutions. In Sri Lanka, however, we have seen ODL become a marketplace offering easy to obtain, for-fee qualifications by institutions with little commitment to superior teaching and learning.
Finally, a perusal of the many types of private HEIs and their varied degrees bring to mind another question – how should the private degrees, provided by state institutions (that are not educational institutions), be regulated? Who should do so?
All of these create a host of problems for the public – for hopeful students and parents and trusting employers. For the higher education sector, recruitment of academic staff, too, has become difficult due to this plethora of ambiguous higher education qualifications, as I discussed in a previous Kuppi article (‘Recruiting academics to state universities’).
Some issues in private HEIs – a bellwether for change in state universities
In this second part of this article, I will discuss some aspects of work in private HEIs – albeit the more established institutions – given that such issues may appear in reform agendas in future.
Across state universities, all permanent staff of a specific category are paid according to the same criteria. The picture is not so clear when it comes to private HEIs since they are different entities legally, typically companies. Private HEIs have salary scales and financial incentives that are different to each other. The more established private HEIs reportedly have attractive renumeration packages, possibly a reason for academics of state universities migrating eagerly to such institutions during sabbatical years and on retirement. This may not of course be the case with other less established, or improperly registered HEIs of which we know little. Academic staff of these more accepted private HEIs seem to value the high financial remuneration they receive (in comparison to state universities) as something that makes their work rewarding.
Attractive remuneration is important to sustain the good life and is at times seen as the institution’s way of encouraging good work. Yet, this has implications for the future of the institution: to continue to deliver on promised financial packages, institutions must continue to have large profit margins. One strategy has been to enroll multiple cohorts of students per year, even up to three or four intakes per year. This can result in exploitative work conditions, since staff must cater to all these cohorts in that same year. If there is inadequate staff, employees are further burdened. On the other hand, if there is a sudden drop in enrolments (degrees can go out of fashion) unexpected layoffs occur. Similar to other sectors that employ short-term contract staff – including state universities – in private HEIs, too, individual teachers, who are on short term contracts that need regular renewal, can feel pressured to work under difficult or exploitative conditions.
At the same time, even in the more established private HEIs, work norms differ from those of state universities in that they include promotional work that keeps the institution’s name in the eye of the public. The Marketing (or similarly named) unit comes up in conversations as one of the most important departments. It appears to weigh in on decision-making related to the number of staff, the amount of re-sits per exams, and other pedagogically important matters. This is a worrying example of how financial rationales interfere with pedagogically or academically sound processes, resulting in problematic results in the classroom. On the plus side, junior colleagues, who had experience in both state and private HEIs, also felt that they faced less harassment in private HEIs – primarily due to the private HEIs ability to take swift action in reported cases of harassment. This is a real indictment on state institutions and their reluctance to address chronic issues of harassment in our universities.
Yet, while we hear much about problems in state universities, we hardly hear of problems that staff in private HEIs face. One rationale for a lack of public expressions by staff is that expressions of discontent might lead to trouble given the importance of reputation for private HEIs. The worry about reputational damage is a growing concern in state universities, too, as evidenced by social media policies and internal conversations on reputational damage, consequent to negative publicity. Institutional worries of reputational damage are harmful in the long run since these impact not only freedom of expression by student and staff, but also research that is possible in and about the education sector.
Some thoughts at the end…
A close look at the private higher education sector is important given its strong presence in the country. Impending reform needs to regulate this diverse array of higher education offerings in the private sector, as well as the state institutions that offer privately-funded options of higher education (a topic for a separate Kuppi on its own). It is time we carefully considered how to build a whole system of higher education out of this broken mess.
Kaushalya Perera is a senior lecturer at the University of Colombo.
Kuppi is a politics and pedagogy happening on the margins of the lecture hall that parodies, subverts, and simultaneously reaffirms social hierarchies.

Singer Nish Peiris is set to take the next big step in her music journey.
The talented vocalist, who has been seen and heard in the scene here for a short while, and was also featured with the now-defunct band, Inner Vision, has announced that she will be fully committing to her solo career, after completing her degree this year.
“I’m finishing my degree this year, and after that I’ll be fully committing to my solo music career,” Nish told The Island.
“I’ve already got a few tours lined up for next year, so I’m really excited for what’s ahead.”
Fans, no doubt, will remember Nish for her smooth voice and stage presence, and the good news is that she is now ready to chart her own path and bring new music to audiences at home and abroad.
With tours already planned for 2027, the year 2026 promises to be an exciting year for the young artiste as she steps into the spotlight on her own.
We wish Nish every success in this new chapter!

 While Sri Lankan music lovers, in Dubai, are eagerly looking forward to being a part of the action on Saturday, 25th July, with Rajiv Sebastian in the limelight, Sri Lankans, in Toronto, Canada, are equally excited and are anxiously awaiting the arrival of Sri Lanka’s famous singer/entertainer Sohan Weerasinghe.
While Sri Lankan music lovers, in Dubai, are eagerly looking forward to being a part of the action on Saturday, 25th July, with Rajiv Sebastian in the limelight, Sri Lankans, in Toronto, Canada, are equally excited and are anxiously awaiting the arrival of Sri Lanka’s famous singer/entertainer Sohan Weerasinghe.
Having done the needful with The X-Periments, the legendary performer has now embarked on an exciting new chapter – a solo career – and Toronto, Canada, will see him do the needful, on Friday, 31st July, 2026, from 8.00 pm to 12.00 am, at the Angus Glen Golf Club.

Sohan Weerasinghe: In Canada, and ready to do the needful on 31st July
Reports indicate that it’s a ‘sold out’ event – naturally with Sohan in the spotlight.

Gamini Hemalal: Creating all the excitement for Sri Lankans in Toronto
Having built his reputation through years of unforgettable performances, and hits that became part of our musical fabric, Sohan is ready to bring his own vision, sound, and stories directly to the audience, in Toronto, Canada, backed by the phenomenal Toronto Ceymphony Live Band.
Says Gamini Hemalal, who has been instrumental in reviving the Sri Lankan entertainment scene, in that part of the world:
“The countdown begins for the most exclusive musical event of the summer! Join us for a premium night of incredible music, elite hospitality, and a lavish buffet as the legendary Sohan Weerasinghe takes the stage live in Toronto!
“This is a high-end event, designed for those who appreciate exceptional entertainment and great food.”
Gamini, who is also a member of the Toronto Ceymphony Live Band, mentioned that it’s going to be an intimate musical evening with the celebrated Sohan Weerasinghe.
From packed auditoriums to intimate shows, Sohan continues to prove why he remains one of Sri Lanka’s most beloved entertainers.
For decades, Sohan Weerasinghe has been a household name in Sri Lankan entertainment.
Known for his captivating smooth voice and charismatic stage presence, Canada will experience it all on Friday, 31st July.
Next on the list of events, Gamini Hemal is working on, is Halloween night and he says “what we plan to do will be very interesting and unique … with a surprise guest star, as well!”

Trump slaps 50% tariffs on Canada and Carney vows to ‘intensify’ trade talks

Showers will occur in the Western, Sabaragamuwa and North-western provinces and in Kandy, Nuwara-Eliya, Galle and Matara districts

Move to extend judges’ retirement ages could damage Sri Lanka’s global image, warns Prof. Peiris

Dengue surge infects 76,000, claims about 53 lives

SC dismisses challenge to gender change procedures

BASL urges Justice Minister not to amend Constitution to increase retirement ages of superior court judges

‘Dates have the highest sugar content to fight Coronavirus’

Sunday Island 27 December – Headlines

#SundayIsland 17th December – Headlines

Sunday Island – 28th March

Sunday Island Headlines – 21 March

Sunday Island – 21st February – Headlines
-

 Business2 days ago
Business2 days ago‘Giving up was never an option’: The fisherman who fought back after losing millions in SL
-

 Features2 days ago
Features2 days agoTwo memorable excerpts from a former SLAF commander’s memoir
-

 Latest News3 days ago
Latest News3 days agoDavis cup Asia/Oceania Group IV 2026 to be held in Colombo from 20th to 25th July
-

 Features2 days ago
Features2 days agoErdoğan’s New Republic
-

 Life style2 days ago
Life style2 days agoTaste of the Swiss Alps comes to Colombo
-
 Features6 days ago
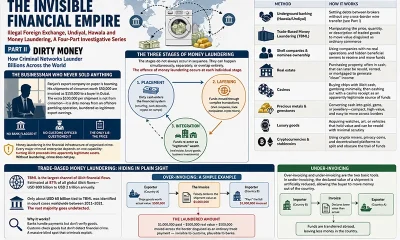
Features6 days agoDirty Money
-

 News3 days ago
News3 days agoDengue outbreak gallops ahead: Infections surpasses 73,455, leaving 50 dead
-

 News3 days ago
News3 days agoEvidence recorded in money laundering case against Yoshitha Rajapaksa