Features
The doctor’s dilemma

It was not just yesterday, or the day before, that this subject was discussed. In fact, it was over a century ago that George Bernard Shaw, the famous Irish playwright, wrote the play, ‘The Doctor’s Dilemma’ that was first staged in 1906. It was published in book-form in 1909. It was considered a ‘problem play’ – a form of drama that emerged during the 19th century, dealing with contentious social issues which were debated on stage.
Would you believe that ‘The Doctor’s Dilemma’ was about moral dilemmas created by limited medical resources and the conflicts between the demands of private medicine as a business and as a vocation?
What do we see today? Not much seems to have changed between the early 1900s in England and the present day in Sri Lanka.
The whole nation now knows that of Dr. Maheshi Wijeratne, specialist neurosurgeon and consultant to the Sri Jayawardenepura Teaching Hospital (SJP TH), has been arrested, remanded and released on bail by the Chief Magistrates Court, Colombo, on a complaint filed by the Commission to Investigate Allegations of Bribery and Corruption (CIABOC). The arrest and remanding has disturbed a hornet’s nest, not only in the social media, amongst patients and elite societal circles, but also, significantly within the medical community.
What is disturbing to me, having been a medical teacher for nearly 45 years and a medical ethicist for many decades, is the lack of clarity amongst the doctors about Dr. Maheshi Wijeratne’s purported offence. This is the current doctors’ dilemma that I have been keenly observing and the main reason for this short essay.
According to reports circulating in the media, a few doctors have resigned from the SJP TH. An unexpected consequence of this has been, according to news items in the mainstream and social media, that doctors at SJP Hospital, and elsewhere, have refused to issue prescriptions to patients, or next of kin, for purchase of drugs, or other required items in the open market, for fear of being arrested. Is this reaction of some doctors in the Ministry of Health (MoH) a ‘healthy trend’? It is said that it is out of a genuine concern, and worry, that what they were doing routinely before, will now be construed to be “corruption”. Or, is it a collective response against the initiative taken by the CIABOC in solidarity with the plight of Dr. Maheshi Wijeratne? Or could it be a sense of ‘collective guilt’?
This fallout has/would jeopardise the health and lives of patients seeking treatment from SJP TH and other State sector hospitals.
Is this reaction by the doctors a reasonable reaction? Or is it an exaggerated knee-jerk response that would be seen by many doctors, as well as the public, as a surreptitious collective attempt in defence of Dr. Maheshi Wijeratne?
The Health Minister, Dr. Nalinda Jayatissa’s attempt to defuse the situation, and, maybe, prevent a nationwide move to embarrass the government and the Health Ministry, may have not have had the desired effect.
Understandably, the arrest of Dr. Maheshi Wijeratne came at a bad time when the antics of the former Health Minister Rambukwella and his family, and the then Secretary/Health, have resulted in them being repeatedly under remand custody and now being indicted on charges of unlawfully acquiring assets. The Rambukwella family case is much clearer and leaves little to the imagination and should not be used in comparison with the neurosurgeon’s case.
It also must be remembered that this is certainly not the first time that Dr. Maheshi Wijertne has literally “hit the headlines”. Her actions as a doctor, quite apart from being a neurosurgeon, regarding the Duminda Silva case, has been much criticised.
I believe that the issues of her serious ‘conflict of interest’ in this case would be a very useful vignette/case study/scenario in the teaching/learning programmes in medical ethics in the years to come.
To return to the issue at hand – i.e., the refusal of some specialists/doctors to give prescriptions for medicines and other purchases from “outside”, l think is counterproductive. The doctors seem to have behaved in an excessive demonstration of “protectionism”. A more circumspect, logical and analytical approach has been taken by the Association of Medical Specialists (AMS) in their letter to the Health Minister.
It must be remembered that specialists giving prescriptions to patients for purchases from “outside” is nothing new. And there have been no previous incidents of arrests and remanding for the same. Even though reliable stories are many in the past of specialists having “deals” with pharmacies, private laboratories and medical device providers.
We need to accept that the arrest and detention of Dr. Maheshi Wijeratne was an event that was waiting to happen for many years! It is an exceptional case and certainly not the norm. Why should honest, bona fide doctors and specialists, who have been genuine in their prescriptions, be perturbed? Surely, the CIABOC will not hound honest doctors doing their duty by their patients? Only those specialists who have been in league with private sector providers of special medicines (especially in oncology) and of medical devices (stents in cardiology) need be disturbed. They, certainly, have cause for concern. Their conscience will be troubling them now, since they are prone to be ‘next on the list’.
In this context, please allow me to digress, albeit briefly, into the worldwide phenomenon of ‘conflict of interest’ between the doctor and the pharmaceutical industry – the ‘Big Pharma’.
To understand the fundamental contradiction between doctors and the drug industry, one must realise that the medical profession has to place patients before self and should work for the maximum benefit of the patient (the concept of fidelity). Beneficence (doing good) or at least, non-maleficence (doing no harm) are other guiding principles. In addition, doctors today are expected to engage in the advocacy for patients – identifying their needs and working for developments in human and physical resource allocations for improvement in healthcare delivery.
In contrast, in the pharmaceutical industry, the guiding principle is profit; research and development of new drugs based on not need, but market demand and profit; research to be the market-leader for profit; service and charity with a view to societal acceptance and development of benevolent institutional images for profit. Some may consider this too harsh a formulation, but I believe this to be a realistic assessment of the present condition.
The relationship between the doctor and the pharmaceutical industry is necessary, unavoidable, but ethically controversial. Furthermore, the public have a right to be concerned if they feel that professional advice offered to them may have been influenced by financial or other benefits offered to medical professionals by commercial interests. The British Medical Association in its publication ‘Philosophy and Practice of Medical Ethics‘ observes that “The medical profession has an obligation to assure the public that treatment offered is appropriate and is justified by its intrinsic merit, uninfluenced by commercial or financial interests. This is especially important in relation to pharmaceutical products.”.
From the innumerable conversations I have had on this subject with many medical colleagues, I have the impression that they tend to believe that doctors are in control of the relationship between them and the drug companies. This sense of ‘well-being’ is near universal among the medical fraternity. In a study done in the Department of Medicine, University of California, in San Francisco, only 39% admitted that “industry promotions and contacts influenced their own prescribing”, but ironically, “84% believed that other doctors’ prescribing was affected”. In other words, the well-researched phenomenon of ‘actor-observer bias’ – that is, the belief that “others are more susceptible to temptation…” than you are – was clearly seen.
Some analysts of this relationship believe that it is the ‘naivety of the medical professional’ to not know that the marketing strategies of pharmaceutical companies are well researched. Paul Witkowski, Director of Pharmacy at Alliance, Ohio, USA, goes further. He says that “Every word and action of pharmaceutical sales representatives has been carefully choreographed and examined in front of ‘reactor panels’ in order to make the best impact of their product in the limited amount of ‘fact time’ they are permitted by their physician
customers. It is extremely successful; that’s why they do it.”
The doctors are showered with biased drug literature and free samples of medicines. This can be considered to relate directly to information transfer to the physicians. What is of greater concern is that ‘gifts’ are given to doctors to influence their prescription practices. These include anything from prescription pads, pens, paperweights to personalised executive diaries and annual subscriptions to medical journals and even to ‘Newsweek’ or ‘Time’ magazine; from sponsoring medical symposia and connected social events, organised by medical associations; with dinner invitations to 5-star hotels; to all expense paid trips abroad to attend international medical conventions.
These are but a few of the temptations that even ethical and honest doctors face in the ‘World of Global Medicine’ today. This, I believe, is the most predominant dilemma that all doctors, the world over, are confronted with.
But what about the deliberately dishonest doctors? Those without any empathy (or even sympathy or compassion) will exploit a patient and extract as much money as they can. These are the doctors who have ‘deals’ with suppliers and providers of medicines and devices. What of them? They are also a cross-section of any society. It is for the general public, the patients, honest and ethical doctors and also the CIABOC and other agencies to help society to separate the grain from the chaff. So that society will uphold the grain and discard the chaff from society. We need ‘whistleblowers’ within our medical community. This cannot be done if too many in the medical community, almost reflexively, become protective – irrespective of the specificity of a given situation. In our country, the Law, based on Roman Dutch Law and English Common Law, ensures that any accused is innocent until proven guilty. Hence, Dr. Maheshi Wijeratne will remain innocent until her case is completed and the judgement is given.
I strongly believe that we, medical professionals, need to be on the right side of the medical ethical divide even in the most difficult of circumstances, and not, in our short-sighted and anxious haste, be on the ‘other’ side.
We, as medical professionals, must not be seen as “protectionist” in the face of serious allegations of financial misdemeanors, corruption or frauds perpetrated against patients. Unconscionable margins (profits) between the purchaser and the seller is unacceptable in any commercial transaction. This becomes grossly unacceptable when doctors are sometimes seen to play intermediary ‘business’ roles between the two.
Let the Law take its course. It will take its time. The hype and sensationalism will soon die out. Dr. Maheshi Wijeratne has every right to her defence without too many flash bulbs and news-hounds. Life will return to normal. I hope where medical professionals are concerned, it will be a ‘new normal’. Will it come to pass? Or will it soon be ‘back to the status quo’?
To paraphrase a famous saying attributed to the Greeks, “The mills of justice grind slowly, but it grinds exceedingly small”.
I know that what I have stated here may not be taken too kindly by some of my professional colleagues.
So be it!
by Dr. Susirith Mendis ✍️
Emeritus Professor
University of Ruhuna
(susmend2610@gmail.com)

Exchanging greetings and resolving to do something positive in the coming year certainly create an uplifting atmosphere. Unfortunately, their effects wear off within the first couple of weeks, and most of the resolutions are forgotten for good. However, this time around, we must be different, because the nation is coming out of the most devastating natural disaster ever faced, the results of which will impact everyone for many years to come. Let us wish that we as a nation will have the courage and wisdom to resolve to do the right things that will make a difference in our lives now and prepare for the future. The truth is that future is going to be challenging for tropical islands like ours.
We must not have any doubts about global warming phenomenon and its impact on local weather patterns. Over its 4.5-billion-year history, the earth has experienced drastic climate changes, but it has settled into a somewhat moderate condition characterised by periods of glaciation and retreat over the last million years. Note that anatomically modern Homo sapiens have been around only for two to three hundred thousand years, and it is reasoned that this stable climate may have helped their civilisation. There have been five glaciation periods over the last five hundred thousand years, and these roughly hundred-thousand-year cycles are explained by the astronomical phenomenon known as the Milankovitch Cycle (the lows marked with stars in Figure 1). At present, the earth is in an inter glacial period and the next glaciation period will be in about eighty thousand years.
 (See Figure 1. Glaciation Cycles)
(See Figure 1. Glaciation Cycles)
During these cycles, the global mean temperature has changed by about 7-8 degrees Centigrade. In contrast to this natural variation, earth has been experiencing a rapid temperature increase over the past hundred years. There is ample scientific evidence from multiple sources that this is caused by the increase in carbon dioxide gas in the atmosphere, which has seen a 50% increase over the historical levels in just hundred years (Figure 2). Carbon dioxide is one of the greenhouse gases which traps heat from the sun and slows the natural cooling process of the earth. This increase of carbon dioxide is due to human activities: fossil fuel burning, industrial processes, deforestation, and agricultural practices. Ironically, those who suffer from the consequences did not contribute to these changes; those who did contribute are trying their best to convince the world that the temperature changes we see are natural, and nothing should be done. We must have no illusions that global warming is a human-caused phenomenon, and it has serious repercussions.
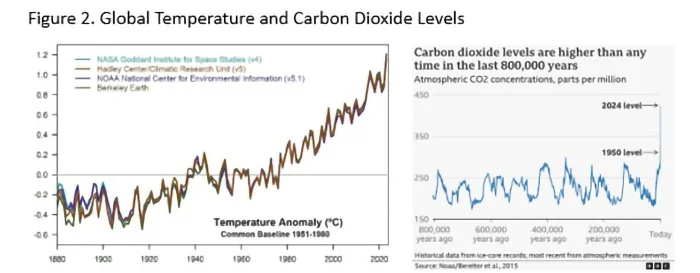
(See Figure 2. Global Temperature and Carbon Dioxide Levels)
Why should we care about global warming? Well, there are many reasons, but let us focus on earth’s water cycle. Middle schoolers know that water evaporates from the oceans, rises into the atmosphere where it cools, condenses, and falls back onto earth as rain or snow. When the oceans warm, the evaporation increases, and the warmer atmosphere can hold more water vapour. Water laden atmosphere results in severe and erratic weather. Ironically, water vapour is also a greenhouse gas, and this has a snowballing effect. The increased ocean temperature also disrupts ocean currents that influence the weather on land. The combined result is extreme and severe weather: violent storms and droughts depending on the geographic location. What is happening on the West coast of the USA is an example. The net result will be major departures from what is considered normal weather over millennia.
International organisations have been talking for 30 years about limiting global temperature increase to 1.5oC above pre-industrial levels by curtailing greenhouse gas emissions. But not much has been done and the temperature has risen by 1.2oC already. The challenge is that even if we can stop greenhouse gas emissions completely, right now, we have the problem of removing already existing 2,500 billion tons of carbon from the atmosphere, for which there are no practical solutions yet. Scientists worry about the consequences of runaway temperature increase and its effect on human life, which are many. It is not a doomsday prediction of life disappearing from earth, but a warning that life will be quite different from what humans are used to. All small tropical nations like ours are burdened with mitigating the consequences; in other words, get ready for more Ditwahs, do not wait for the twelve-day forecast.
Some opined that not enough warning was given regarding Ditwah; the truth is that the tools available for long-term prediction of the path or severity of a weather event (cyclone, typhoon, hurricane, tornado) are not perfect. There are multitude of rapidly changing factors contributing to the behavior of weather events. Meteorologists feed most up to date data to different computer models and try to identify the prediction with the highest probability. The multiple predictions for the same weather event are represented by what is known as spaghetti plots. Figure 3 shows the forecasted paths of a 2019 Atlantic hurricane five days ahead on the right and the actual path it followed on the left. While the long-term prediction of the path of a cyclone remains less accurate, its strength can vary within hours. There are several Indian ocean cyclones tracking sites online accessible to the public.

Figure 3. Forecasting vs Reality
There is no argument that short-term forecasts of this nature are valuable in saving lives and movable assets, but having long term plans in place to mitigate the effects of natural disasters is much more important than that. If a sizable section of the population must start over their lives from ground zero after every storm, how can a country economically develop?
The degree of our unpreparedness came to light during Ditwah disaster. It is not for lack of awareness; judging by the deluge of newspaper articles, blogs, vlogs, and speeches made, there is no shortage of knowledge and technical expertise to meet the challenge. The government has assured the necessary resources, and there is good reason to trust that the funds will be spent properly and not to line the pockets as happened during previous disasters. However, history tells us that despite the right conditions and good intentions, we could miss the opportunity again. Reasons for such skepticisms emerged during the few meetings the President held with the bureaucrats while visiting effected areas. Also, the COPE committee meetings plainly display the inherent inefficiencies and irregularities of our system and the absence of work ethics among all levels of the bureaucracy.
What it tells us is that we as a nation have an attitude problem. There are ample scholarly analyses by local as well as international researchers on this aspect of Sri Lankan psyche, and they label it as either island or colonial mentality. The first refers to the notion of isolated communities perceiving themselves as exceptional or superior to the rest of the world, and that the world is hell-bent on destroying or acquiring what they have. This attitude is exacerbated by the colonial mentality that promoted the divide and conquer rules and applied it to every societal characteristic imaginable; and plundered natural resources. As a result, now we are divided along ethnic, linguistic, religious, political, class, caste, geography, wealth, and many more real and imagined lines. Sadly, politicians, some religious leaders, and other opportunists keep inflaming these sentiments for their benefit when most of the population is willing to move on.
The first wish, therefore, is to get the strength, courage, and wisdom to think rationally, and discard outdated and outmoded belief systems that hinder our progress as a nation. May we get the courage to stop venerating elite who got there by exploiting the masses and the country’s wealth. More importantly, may we get the wisdom to educate the next generation to be free thinkers, give them the power and freedom to reject fabrications, myths, and beliefs that are not based on objective facts.
This necessitates altering our attitude towards many aspects of life. There is no doubt that free thinking does not come easily, it involves the proverbial ‘exterminating the consecrated bull.’ We are rightfully proud about our resplendent past. It is true that hydraulic engineering, art, and architecture flourished during the Anuradhapura period.
However, for one reason or another, we have lost those skills. Nowadays, all irrigation projects are done with foreign aid and assistance. The numerous replicas of the Avukana statue made with the help of modern technology, for example, cannot hold a candle to the real one. The fabled flying machine of Ravana is a figment of marvelous imagination of a skilled poet. Reality is that today we are a nation struggling with both natural and human-caused disasters, and dependent on the generosity of other nations, especially our gracious neighbor. Past glory is of little help in solving today’s problems.
Next comes national unity. Our society is so fragmented that no matter how beneficial a policy or an idea for the nation could be, some factions will oppose it, not based on facts, but by giving into propaganda created for selfish purposes. The island mentality is so pervasive, we fail to trust and respect fellow citizens, not to mention the government. The result is absence of long-term planning and stability. May we get the insight to separate policy from politics; to put nation first instead of our own little clan, or personal gains.
With increasing population and decreasing livable and arable land area, a national land management system becomes crucial. We must have an intelligent zoning system to prevent uncontrolled development. Should we allow building along waterways, on wetlands, and road easements? Should we not put the burden of risk on the risk takers using an insurance system instead of perpetual public aid programs? We have lost over 95% of the forest cover we had before European occupation. Forests function as water reservoirs that release rainwater gradually while reducing soil erosion and stabilizing land, unlike monocultures covering the hill country, the catchments of many rivers. Should we continue to allow uncontrolled encroachment of forests for tourism, religious, or industrial purposes, not to mention personal enjoyment of the elite? Is our use of land for agricultural purposes in keeping with changing global markets and local labor demands? Is haphazard subsistence farming viable? What would be the impact of sea level rising on waterways in low lying areas?
These are only a few aspects that future generations will have to grapple with in mitigating the consequences of worsening climate conditions. We cannot ignore the fact that weather patterns will be erratic and severe, and that will be the new normal. Survival under such conditions involves rational thinking, objective fact based planning, and systematic execution with long term nation interests in mind. That cannot be achieved with hanging onto outdated and outmoded beliefs, rituals, and traditions. Weather changes are not caused by divine interventions or planetary alignments as claimed by astrologers. Let us resolve to lay the foundation for bringing up the next generation that is capable of rational thinking and be different from their predecessors, in a better way.
by Geewananda Gunawardana

For centuries, Sri Lanka’s biological knowledge travelled the world — anonymously. Embedded deep within the pages of European natural history books, Sinhala words were copied, distorted and repurposed, eventually fossilising into Latinised scientific names of snakes, bats and crops found thousands of kilometres away.
Africa’s reptiles, Europe’s taxonomic catalogues and global field guides still carry those echoes, largely unnoticed and uncredited.
Now, a Sri Lankan herpetologist is tracing those forgotten linguistic footprints back to their source.
Through painstaking archival research into 17th- and 18th-century zoological texts, herpetologist and taxonomic researcher Sanjaya Bandara has uncovered compelling evidence that several globally recognised scientific names — long assumed to be derived from Greek or Latin — are in fact rooted in Sinhala vernacular terms used by villagers, farmers and hunters in pre-colonial Sri Lanka.
“Scientific names are not just labels. They are stories,” Bandara told The Island. “And in many cases, those stories begin right here in Sri Lanka.”

Sanjaya Bandara
At the heart of Bandara’s work is etymology — the study of word origins — a field that plays a crucial role in zoology and taxonomy.
While classical languages dominate scientific nomenclature, his findings reveal that Sinhala words were quietly embedded in the foundations of modern biological classification as early as the 1700s.
One of the most striking examples is Ahaetulla, the genus name for Asian vine snakes. “The word Ahaetulla is not Greek or Latin at all,” Bandara explained. “It comes directly from the Sinhala vernacular used by locals for the Green Vine Snake.” Remarkably, the term was adopted by Carl Linnaeus himself, the father of modern taxonomy.
Another example lies in the vespertilionid bat genus Kerivoula, described by British zoologist John Edward Gray. Bandara notes that the name is a combination of the Sinhala words kiri (milky) and voula (bat). Even the scientific name of finger millet, Eleusine coracana, carries linguistic traces of the Sinhala word kurakkan, a cereal cultivated in Sri Lanka for centuries.
Yet Bandara’s most intriguing discoveries extend far beyond the island — all the way to Africa and the Mediterranean.
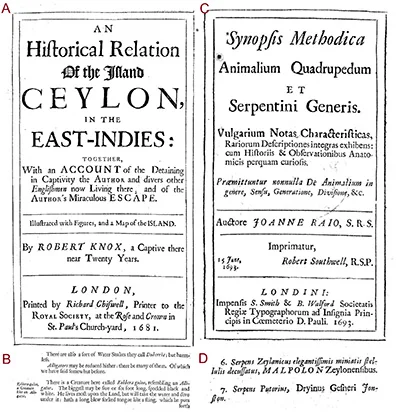
In a research paper recently published in the journal Bionomina, Bandara presented evidence that two well-known snake genera, Duberria and Malpolon, both described in 1826 by Austrian zoologist Leopold Fitzinger, likely originated from Sinhala words.
The name Duberria first appeared in Robert Knox’s 1681 account of Ceylon, where Knox refers to harmless water snakes called “Duberria” by locals. According to Bandara, this was a mispronunciation of Diyabariya, the Sinhala term for water snakes.
“Mispronunciations are common in Knox’s writings,” Bandara said. “English authors of the time struggled with Sinhala phonetics, and distorted versions of local names entered European literature.”
Over time, these distortions became formalised. Today, Duberria refers to African slug-eating snakes — a genus geographically distant, yet linguistically tethered to Sri Lanka.
Bandara’s study also proposes the long-overdue designation of a type species for the genus, reviving a 222-year-old scientific name in the process.
Equally compelling is the case of Malpolon, the genus of Montpellier snakes found across North Africa, the Middle East and southern Europe. Bandara traced the word back to a 1693 work by English zoologist John Ray, which catalogued snakes from Dutch India — including Sri Lanka.
“The term Malpolon appears alongside Sinhala vernacular names,” Bandara noted. “It is highly likely derived from Mal Polonga, meaning ‘flowery viper’.” Even today, some Sri Lankan communities use Mal Polonga to describe patterned snakes such as the Russell’s Wolf Snake.
Bandara’s research further reveals Sinhala roots in the African Red-lipped Herald Snake (Crotaphopeltis hotamboeia), whose species name likely stems from Hothambaya, a regional Sinhala term for mongooses and palm civets.
“These findings collectively show that Sri Lanka was not just a source of specimens, but a source of knowledge,” Bandara said. “Early European naturalists relied heavily on local names, local guides and local ecological understanding.”
 Perhaps the most frequently asked question Bandara encounters concerns the mighty Anaconda. While not a scientific name, the word itself is widely believed to be a corruption of the Sinhala Henakandaya, another snake name recorded in Ray’s listings of Sri Lankan reptiles.
Perhaps the most frequently asked question Bandara encounters concerns the mighty Anaconda. While not a scientific name, the word itself is widely believed to be a corruption of the Sinhala Henakandaya, another snake name recorded in Ray’s listings of Sri Lankan reptiles.
“What is remarkable,” Bandara reflected, “is that these words travelled across continents, entered global usage, and remained there — often stripped of their original meanings.”
For Bandara, restoring those meanings is about more than taxonomy. It is about reclaiming Sri Lanka’s rightful place in the history of science.
“With this study, three more Sinhala words formally join scientific nomenclature,” he said.
“Who would have imagined that a Sinhala word would be used to name a snake in Africa?”
Long before biodiversity hotspots became buzzwords and conservation turned global, Sri Lanka’s language was already speaking through science — quietly, persistently, and across continents.
By Ifham Nizam

However, the children and their needs may be forgotten after a disaster.
Do not forget that children will also experience fear and distress although they may not have the capacity to express their emotions verbally. It is essential to create child-friendly spaces that allow them to cope through play, draw, and engage in supportive activities that help them process their experiences in a healthy manner.
The Institute for Research & Development in Health & Social Care (IRD), Sri Lanka launched the campaign, titled “Children first,” after the 2004 Tsunami, based on the fundamental principle of not to medicalise the distress but help to normalise it.

The Island picture page
The IRD distributed drawing material and play material to children in makeshift shelters. Some children grabbed drawing material, but some took away play material. Those who choose drawing material, drew in different camps, remarkably similar pictures; “how the tidal wave came”.
“The Island” supported the campaign generously, realising the potential impact of it.
The campaign became a popular and effective public health intervention.
“A public health intervention (PHI) is any action, policy, or programme designed to improve health outcomes at the population level. These interventions focus on preventing disease, promoting health, and protecting communities from health threats. Unlike individual healthcare interventions (treating individuals), which target personal health issues, public health interventions address collective health challenges and aim to create healthier environments for all.”
The campaign attracted highest attention of state and politicians.
The IRD continued this intervention throughout the protracted war, and during COVID-19.
The IRD quick to relaunch the “children first” campaign which once again have received proper attention by the public.
While promoting a public health approach to handling the situation, we would also like to note that there will be a significant smaller percentage of children and adolescents will develop mental health disorders or a psychiatric diagnosis.
We would like to share the scientific evidence for that, revealed through; the islandwide school survey carried out by the IRD in 2007.
 During the survey, it was found that the prevalence of emotional disorder was 2.7%, conduct disorder 5.8%, hyperactivity disorder was 0.6%, and 8.5% were identified as having other psychiatric disorders. Absenteeism was present in 26.8%. Overall, previous exposure to was significantly associated with absenteeism whereas exposure to conflict was not, although some specific conflict-related exposures were significant risk factors. Mental disorder was strongly associated with absenteeism but did not account for its association with tsunami or conflict exposure.
During the survey, it was found that the prevalence of emotional disorder was 2.7%, conduct disorder 5.8%, hyperactivity disorder was 0.6%, and 8.5% were identified as having other psychiatric disorders. Absenteeism was present in 26.8%. Overall, previous exposure to was significantly associated with absenteeism whereas exposure to conflict was not, although some specific conflict-related exposures were significant risk factors. Mental disorder was strongly associated with absenteeism but did not account for its association with tsunami or conflict exposure.
The authors concluded that exposure to traumatic events may have a detrimental effect on subsequent school attendance. This may give rise to perpetuating socioeconomic inequality and needs further research to inform policy and intervention.
Even though, this small but significant percentage of children with psychiatric disorders will need specialist interventions, psychological treatment more than medication. Some of these children may complain of abdominal pain and headaches or other physical symptoms for which doctors will not be able to find a diagnosable medical cause. They are called “medically unexplained symptoms” or “somatization” or “bodily distress disorder”.
Sri Lanka has only a handful of specialists in child and adolescent psychiatric disorders but have adult psychiatrists who have enough experience in supervising care for such needy children. Compared to tsunami, the numbers have gone higher from around 20 to over 100 psychiatrists.
Most importantly, children absent from schools will need more close attention by the education authorities.
In conclusion, going by the principles of research dissemination sciences, it is extremely important that the public, including teachers and others providing social care, should be aware that the impact of Cyclone Ditwah, which was followed by major floods and landslides, which is a complex emergency impact, will range from normal human emotional behavioural responses to psychiatric illnesses. We should be careful not to medicalise this normal distress.
It’s crucial to recall an important statement made by the World Health Organisation following the Tsunam
Prof. Sumapthipala MBBS, DFM, MD Family Medicine, FSLCFP (SL), FRCPsych, CCST (UK), PhD (Lon)]
Director, Institute for Research and Development in Health and Social Care, Sri Lanka
Emeritus Professor of Psychiatry, School of Medicine, Faculty of Medicine & Health Sciences, Keele University, UK
Emeritus Professor of Global Mental Health, Kings College London
Secretary General, International society for Twin Studies
Visiting Professor in Psychiatry and Biomedical Research at the Faculty of Medicine, Kotelawala Defence University, Sri Lanka
Associate Editor, British Journal Psychiatry
Co-editor Ceylon Medical Journal.
Prof. Athula Sumathipala

Navy seizes an Indian fishing boat poaching in northern waters

Mandhana, Shafali and Ghosh help India edge run-fest to go 4-0 up

Showers predicted in several provinces today (29th December)

Delay in govt. response to UK sanctions on ex-military chiefs, and others causes concern

Sri Lanka outlines seven key vectors of international cooperation at Moscow forum

Sri Lanka third most preferred destination for Indians

‘Dates have the highest sugar content to fight Coronavirus’

Sunday Island 27 December – Headlines

#SundayIsland 17th December – Headlines

Sunday Island – 28th March

Sunday Island Headlines – 21 March

Sunday Island – 21st February – Headlines
-

 News7 days ago
News7 days agoMembers of Lankan Community in Washington D.C. donates to ‘Rebuilding Sri Lanka’ Flood Relief Fund
-

 News5 days ago
News5 days agoBritish MP calls on Foreign Secretary to expand sanction package against ‘Sri Lankan war criminals’
-

 Features7 days ago
Features7 days agoGeneral education reforms: What about language and ethnicity?
-

 News7 days ago
News7 days agoSuspension of Indian drug part of cover-up by NMRA: Academy of Health Professionals
-

 Sports5 days ago
Sports5 days agoChief selector’s remarks disappointing says Mickey Arthur
-

 News4 days ago
News4 days agoStreet vendors banned from Kandy City
-

 Editorial7 days ago
Editorial7 days agoA very sad day for the rule of law
-

 News7 days ago
News7 days agoUS Ambassador to Sri Lanka among 29 career diplomats recalled