Features
A Good Guide to the Omicron Variant
By M.C.M. Iqbal, PhD
Despite the WHO adopting a neutral system to name the variants of the coronavirus that keep emerging (using letters of the Greek alphabet), the Omicron variant is associated with South Africa. The last variant of the virus to emerge was the Delta variant, which surfaced in December 2020, in India. There are two more letters between Delta and Omicron in the Greek alphabet that the WHO decided not to use. These are ‘Nu’ and ‘Xie’, which the WHO thought could be confused with ‘new’ while Xie is a common surname in China.
The Omicron variant is spreading in many countries. With the number of infected persons rising and another wave expected, many countries in Europe have imposed the usual methods to arrest the spread, with immediate lockdowns. However, scientists are still collecting data to find out how bad Omicron is, since the data seems to indicate that in South Africa, the disease is not as bad as the Delta variant. At the same time, in Europe, there is no significant change in the number of persons hospitalized. Of immediate concern to health authorities are, is the Omicron variant spreading faster than the earlier variants, does it cause more or less severe disease, and can it bypass the vaccines available?
Discovery
Scientists in South Africa announced on 25 November the discovery of a new variant of the coronavirus. On 26 November, the WHO named it Omicron. Although South Africa has been labeled as the country of origin, the virus was identified in neighbouring Botswana. In addition, there are reports of an earlier detection of this variant in the Netherlands.
PCR tests look for four markers on the virus genome to identify it as the coronavirus. The tests in Botswana showed a reduced sensitivity because one of the four targets was not being detected. These samples were sent to South Africa, where scientists have state-of-the-art facilities to look for changes in the genome of the virus. Changes are found by reading the ‘letters’ of the virus genome (called sequencing) and comparing it to the already available genome of the virus. The new Omicron variant had many more changes than the Delta variant.
Global status
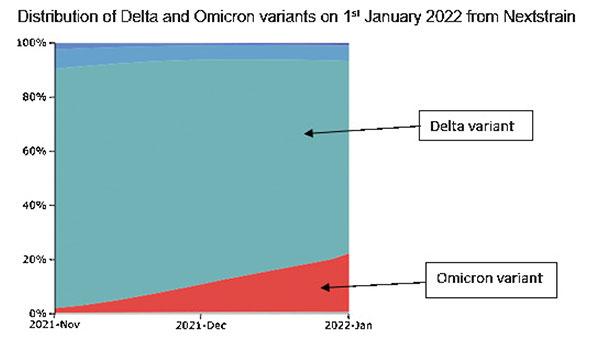
By 14th January, the Omicron variant had spread to 116 countries in all six continents since its discovery on 26 November 2021. The figure below shows the gradual replacement of the presently dominant Delta variant by the Omicron variant; at present global data on the coronavirus, maintained by Nextstrain (https:// nextstrain.org/ncov/open/global) shows a decline of the Delta variant from 88% on 30th October 2021 to 42% on 8th January 2022, while correspondingly the Omicron variant has increased from less than 1% to 56%. Nextstrain is a global database presenting a real-time view of the evolution of the genomes of the coronavirus and other globally important pathogens. The interactive platform provides information to professionals and the public to understand the spread and evolution of pathogens, including information on individual countries.
Distribution of Delta and Omicron variants on 1st January 2022 from Nextstrain. (Please see graph)
What’s unique about Omicron?
Unlike the previous variants of the coronavirus, this variant has over 30 changes (mutations) to its spike (a protein), the characteristic flower-like protrusion on its surface. It was these changes to the spike, one of the four targets of the PCR test that raised alarm bells in Botswana. This spike makes the coronavirus special – it is the key it uses to gain entry into the cells in our throat and lungs. The previous variants, Alpha and Delta also had changes in their spike protein, enabling them to enter cells more efficiently and thus making them more infectious. The vaccines against the virus are based on this spike, and the antibodies produced by our immune system are specific to the spike protein. Thus, any significant changes to the spike means the previous vaccines may not be effective against the newly changed spikes on the Omicron variant.
While the Omicron variant can spread rapidly, it appears to cause milder disease compared to the Alpha and Delta variants. Scientists believe this is because Omicron infects the upper airways or the throat, and not the lungs further down. Based on experiments done on hamsters and mice, scientists found the concentration of the virus was much lower in the lungs than in their throat. The earlier variants of the coronavirus caused severe damage to the lungs of the infected people, with extreme cases needing oxygen. This does not seem to be the case with Omicron. Scientists believe the changes to the spike enables the virus to enter cells in the throat more easily than in the lungs.
It can spread rapidly
The virus is quickly expelled into the air if it infects and multiplies in the throat. Since it causes a milder form of the disease, infected persons may be unaware that they carry the virus. They would be moving about socially and at work, spreading the virus. Thus, the obvious means of slowing or preventing the spread of the virus is to strictly wear the mask at all times, and avoid social gatherings.
Studies have suggested that the period between exposure to the virus and onset of symptoms has also reduced to three days for Omicron. At the pandemic’s beginning, this was more than five days, and for the Delta variant it was four days.
What is of immediate concern?
Of concern to scientists is the better ability of the Omicron to spread rapidly in the population and its suspected ability to bypass our immune system. Our immune system is our internal defense system, using antibodies and an arsenal of chemicals and cells. The available vaccines are designed on the coronavirus variants circulating in the population. Thus, major changes to the coronavirus can reduce the efficiency of the available vaccines. Both these concerns have been observed in the past month: Omicron can spread more rapidly than the presently dominant Delta variant, and observations on vaccinated people show a reduced ability by the vaccines to prevent infections, compared to the Delta variant. This has called for booster doses for people who have already received the two mandatory doses. In Israel, even a fourth vaccination is being administered.
How could the variant have evolved?
 Variants of the coronavirus result from changes to the virus’s genome, called mutations. What is troubling about the Omicron variant is that it has many mutations in its spike. Mutations happen spontaneously as the virus multiplies in our bodies and spreads to others. Thus, the virus gradually accumulates small changes to its advantage. These advantages are infecting us more efficiently, spreading to others more easily, and multiplying more rapidly. Scientists believe that one possibility is that the virus circulated in a small isolated group of people (say a village), piling up the mutations over time, and then escaping into a broader population, and then eventually crossing borders.
Variants of the coronavirus result from changes to the virus’s genome, called mutations. What is troubling about the Omicron variant is that it has many mutations in its spike. Mutations happen spontaneously as the virus multiplies in our bodies and spreads to others. Thus, the virus gradually accumulates small changes to its advantage. These advantages are infecting us more efficiently, spreading to others more easily, and multiplying more rapidly. Scientists believe that one possibility is that the virus circulated in a small isolated group of people (say a village), piling up the mutations over time, and then escaping into a broader population, and then eventually crossing borders.
Another possibility is that it developed in a single individual and spread to others. This happens when a person has low immunity, resulting in a prolonged infection because the immune system cannot eliminate the virus. This leads to the virus developing changes (mutating) to overcome the mild immune response. Answering this question needs scientists to painstakingly reconstruct the history of the virus, using tools from molecular biology. Unfortunately, locating patient zero is difficult since it is impossible to analyze the virus (or sequence its genome) of all the persons infected with the Omicron variant. What is usually possible is to determine a general area or community and the time of origin.
What can we do about it?
Vaccinate! This is the primary tool we have to prevent the spread of the virus and not give it opportunities to multiply. In addition, we should rigorously follow the simple rules we are familiar with – wear the mask when outside, physically distance ourselves, and follow hygienic practices by washing our hands with soap, and avoiding touching our nose and face with possibly contaminated hands.
The good news
The coronavirus has been with us for over two years. Many were infected and have recovered from the virus during this period, providing natural immunity. Others have acquired immunity through vaccinations. When a new variant infects these people, they will manifest a milder form of the disease. This may explain the reduced hospitalisation of Omicron patients.
A booster dose to those already vaccinated or were naturally infected by the coronavirus, appears to provide reasonable protection against the Omicron variant.
And the bad news
The Omicron variant can evade immunity from previous infections. A recent analysis of surveillance data from South Africa, involving over two million persons, indicated suspected reinfections of those previously infected. This is in contrast to Beta and Delta variants, which did not lead to reinfections on such a scale.
The Future
The coronavirus is here for the long haul. Variants will keep emerging, and it seems unlikely it can be eradicated. The media should help counter vaccine hesitancy and the spread of misinformation. As individuals, we need to understand the biology of the virus to avoid spreading the virus and infecting ourselves and others. Science has to be supported in a broad sense to develop strategies by the health authorities and policymakers.
Further reading
S. Wild. How the Omicron variant got so many scary mutations. Scientific American, 3rd December 2021.
Michael Chan Chi-wai.
G. Vogel and K. Kupferschmidt. Early lab studies hint Omicron may be milder. But most scientists reserve judgment. Science, 20th December 2021.
K. Kupferschmidt and G. Vogel. Omicron threats remain fuzzy as cases explode. Science, 7 January 2022.
(The writer is a scientist in Plant and Environmental Sciences, National Institute of Fundamental Studies, Hanthane Road, Kandy. He can be reached at iqbal.mo@nifs.ac.lk)

A quiet yet profound shift is underway in American healthcare, and its implications extend far beyond the United States’ borders. A recent Associated Press report describes a scene that would have seemed improbable, even five years ago: a woman in Texas, experiencing side effects from a weightloss injection, does not call her doctor, visit a clinic, or even search Google. Instead, she opens her phone and consults ChatGPT. She tells the system how she feels, describes her symptoms, and receives an instant explanation. This behaviour, once the domain of early adopters and technology enthusiasts, has now entered the mainstream. A West Health–Gallup poll confirms that nearly onequarter of American adults used an AI tool for health information or advice in the previous month. For a country with one of the world’s most expensive and fragmented healthcare systems, this shift is not merely a technological curiosity. It is a sign of the public searching for speed, clarity, and affordability in a system that often fails to provide any of these.
Sri Lanka, though vastly different in scale, culture, and resources, is not insulated from this global transformation. If anything, the pressures that drive Americans toward AI—long wait times, high costs, difficulty accessing specialists—are even more acute in our own health system. The difference is that Sri Lanka is only beginning to experience the cultural and institutional adjustments that accompany widespread AI use. Yet the trajectory is unmistakable. What is happening in the United States today is almost certainly a preview of what will happen here tomorrow in Sri Lanka, though in a form shaped by our own social realities, linguistic diversity, and healthcare traditions.
The American experience shows that AI is becoming the new gateway to health information. As Dr. Karandeep Singh of UC San Diego observes, AI tools now function as an improved version of the old Google search. Instead of sifting through dozens of links, users receive a concise, conversational summary tailored to their question. This is precisely the kind of convenience that Sri Lankans, too, will find irresistible. In a country where a single specialist appointment can require hours of travel, waiting, and uncertainty, the appeal of an instant, alwaysavailable digital assistant is obvious. The idea that one could ask a question about a rash, a fever, a medication side effect, or a lab report and receive an immediate explanation—without navigating hospital queues or private consultation fees—will inevitably attract public interest. For example, one of my friends, who was with me in school, called me and said he is prescribed Linavic, a drug for type 2 diabetes. I told him that, as it is not widely known in the USA, to give me the generic name. He searched ChatGPT and told me it is called Tradjenta, which is widely available in the USA as a prescription drug for type 2 diabetes.
But Sri Lanka’s path will not be identical to America’s. Our adoption of AI in healthcare is emerging through institutions rather than individuals. Nawaloka Hospitals has already introduced AI-powered chatbots, including NASHA, an OPD assistant capable of guiding patients through symptom assessment and basic triage. This is a significant development because it signals that Sri Lankan hospitals are preparing for a future in which AI is not an optional addon but a core part of patient interaction. The government’s draft National AI Strategy reinforces this direction by identifying healthcare as a priority sector and emphasising responsible, transparent, and safe deployment. Academic bodies, such as the Sri Lanka Medical Association, have also begun training clinicians to understand and work alongside AI systems. These are early but important steps, suggesting that Sri Lanka is building the professional ecosystem needed for safe AI integration.
Yet, the public’s relationship with AI remains limited. Unlike in the United States, where consumers independently experiment with tools like ChatGPT, Sri Lankans tend to rely on doctors as the primary source of authority. Digital literacy varies widely, especially outside urban centres. Sinhala and Tamilcapable AI tools are still developing. And our society has a long history of health misinformation spreading rapidly through social media, from miracle cures to conspiracy theories. Without careful regulation and public education, AI could amplify these risks rather than reduce them. The danger is not that AI will replace doctors, but that poorly informed users may treat AI outputs as definitive diagnoses, bypassing professional care when it is urgently needed.
At the same time, Sri Lankans’ lived experiences reveal why AI will inevitably become part of the healthseeking landscape. Anyone who has visited the outpatient department of a major government hospital knows the reality: queues forming before dawn, patients clutching files and prescriptions, and overworked medical officers trying to see hundreds of cases in a single shift. In rural areas, the situation is even more challenging. A villager in Monaragala or Mullaitivu may have to travel hours to see a specialist, often relying on neighbours or family for transport. Many postpone care simply because they are unsure whether a symptom is serious enough to justify the journey. For such individuals, an AI-based triage tool—available on a basic smartphone, in Sinhala or Tamil—could be transformative. It could help them decide whether to seek immediate care, wait for the next clinic day, or manage the issue at home.
Sri Lanka’s private healthcare sector, too, is ripe for AI integration. Private hospitals are increasingly turning to digital systems for appointment scheduling, lab report delivery, and patient communication. Anyone who has waited for hours at a private OPD, despite having an appointment, knows the frustration. AI-driven systems could help streamline patient flow, predict peak times, and reduce bottlenecks. They could also assist doctors by summarising patient histories, flagging potential drug interactions, and providing evidencebased guidelines. For patients, AI could offer explanations of lab results in simple language, reducing anxiety and improving understanding.
There are already glimpses of this future. Some Sri Lankan patients, especially younger urban professionals, quietly admit that they use AI tools to interpret their blood tests before seeing a doctor.
Others use AI to understand the side effects of medications prescribed to them. Parents use AI to check whether a child’s fever pattern is typical or concerning. Migrant workers, returning home for short visits, use AI to prepare questions for their doctors, ensuring they make the most of limited consultation time. These behaviours mirror the early stages of the American trend, though on a smaller scale.
Sri Lanka’s cultural context will shape how AI is used. Our society places great trust in doctors, often viewing them as authoritative figures whose word should not be questioned. This trust is a strength, but it can also discourage patients from seeking information independently. AI has the potential to shift this dynamic—not by undermining doctors, but by empowering patients to participate more actively in their own care. A patient who understands their condition is better able to follow treatment plans, ask relevant questions, and recognise warning signs. AI can support this empowerment, provided it is used responsibly.
The deeper question is not whether Sri Lanka will adopt AI in healthcare, but how. The American example shows both the promise and the peril. AI can democratise access to information, reduce anxiety, and empower patients. But it can also mislead, oversimplify, or create false confidence. The challenge for Sri Lanka is to build a culture of responsible use—one that recognises AI as a tool, not a substitute for clinical judgment. Hospitals must ensure accuracy and transparency. Regulators must set standards. And the public must learn to treat AI as a guide, not a guru.
Sri Lanka has an opportunity to leapfrog. By studying the American experience, we can avoid its pitfalls and adopt its strengths. We can design AI systems that respect our linguistic diversity, our cultural habits, and our healthcare realities. We can integrate AI into hospitals in ways that enhance, rather than erode, the doctor-patient relationship. And we can prepare our citizens to use these tools wisely, with curiosity but also with caution.
The transformation is already underway. It will accelerate whether we prepare for it or not. The question for Sri Lanka is whether we will shape this future deliberately or allow it to shape us by default. The American shift toward AImediated healthcare is a reminder that technology does not wait for societies to catch up. It moves forward, and nations must decide whether to follow passively or lead thoughtfully. Sri Lanka, with its strong public health tradition and growing technological ambition, has every reason to choose the latter.
by Prof Amarasiri de Silva

I began running on the beach after a fall on a broken pavement left me with a head injury and a surgically repaired eyebrow. Mount Lavinia beach, world‑famous and crowded, especially on Sundays, is only a seven‑minute walk from home, so it became the obvious place for my rehabilitation jogs.
On my first day, my wife, a true Mount Lavinia girl, accompanied me. Though we’ve been married for over 40 years, this was the first time I had ever jogged on the beach. She practically shepherded me there and watched from a safe distance as I made my way towards the Wellawatte breakwater. Dogs were everywhere: some strays, some with collars. I’m not usually afraid of dogs, so I ran past them confidently. Then one fellow barked sharply, making me stop. He advanced even after I stood still. I bent down, picked up some sand, and only then did he retreat, still protesting loudly. On my return run, he repeated the performance.
The next time, I carried a stick. The beach was quiet, perhaps my friend had taken the day off. But on the third day he was back, barking as usual. I showed him the stick and continued. Further along, more dogs barked, and I repeated the ritual. Soon I found myself growing jittery, even numb, whenever I approached a dog. Jogging was no longer comfortable.
My elder daughter, an ardent animal lover who keeps two dogs and wanting to have more, suggested bribery, specifically, biscuits. So, on my next run, I filled my pocket with them. When the usual culprit appeared, I tossed him a biscuit before he could bark. He sniffed suspiciously, then ate it. I jogged on. The rest of the “orchestra” received similar treatment and promptly forgot to bark. Not a dog barked the entire run, or on my way back.
Some groups had five or six dogs, but bribing the noisiest one was enough to quieten the rest. Soon they grew used to me running close to them, and the biscuits made me a trusted friend. These round little sugary crackers turned out to be the perfect currency for seemingly aggressive but essentially harmless dogs, a fact well known to my daughter, Dr. Honda Hitha, but a revelation to me.
One day, a friendly dog decided to escort me home. After receiving his biscuit, he lingered near our gate before returning to the beach. Over time, the number of escorts grew until I found myself flanked by about 10 canine disciples. They became my strength instead of a source of fear. They were darlings. Unlike humans, their affection, even if won initially with biscuits, soon became unconditional.
They still accompany me home, whether or not they receive a treat. Bless them! May they be born human in their next lives, perhaps the only way our wicked world can become a better place.
by Dr. M. M. Janapriya

If there is one country that urgently needs a regime change it is Israel. The whole world is suffering and thousands of people, including children and women, are dying due to Israel’s Prime Minister Benjamin Netanyahu’s political survival strategy. He needs the war to avoid going to jail and also certain defeat at the next elections. The corruption and other charges against him, if proved, would send him to jail. He had asked the Israel President for a pardon and his friend Trump also has written to the President, on his behalf.
Netanyahu is able to commit genocide in Gaza with impunity because the US backs him to the hilt, economically, politically, militarily and also in the United Nations. Without all this, Israel will not be able to fight its many wars and pursue its “Greater Israel” project in Gaza, Lebanon, Syria, and also weaken the countries that oppose its grand plan, such as Iran, Yemen and Turkey. The US gives military aid to Israel, worth USD 3.8 bn, annually, which is used in these genocidal wars and expansionist projects. The US is, therefore, complicit in all these war crimes.
US presidents, beginning from Eisenhower (1950) to Joe Biden (2022), expressed displeasure at Israeli aggression. Ronald Reagan halted the shipment of cluster artillery shells, in 1982, over concerns about their use against civilians in Lebanon, and delayed the delivery of F-16 warplanes until Israel withdrew from Lebanon. George H.W. Bush (1990s) postponed $10 billion in loan guarantees in 1991 to pressure Israel to stop building settlements in the West Bank and to attend the Madrid peace conference. Barack Obama frequently criticised Israeli settlement expansion and, in the final days of his term, withheld a US UN Security Council veto on a resolution regarding settlements. Joe Biden (2020s) threatened to withhold military aid if Israel launched a major offensive in Rafah during the 2024 conflict in Gaza, pausing a shipment of heavy bombs. Most of these presidents had been in favour of the two state solution for the Palestine problem as well.
Trump abandoned these longstanding US policies on Israel that were upheld by Obama and later restored by Biden. Significant and far-reaching changes, included recognising Jerusalem as Israel’s capital, moving the embassy, declaring settlements not inherently illegal, and recognising Golan Heights, which belonged to Syria, as part of Israel sovereignty. These evil deeds of Trump seem to have boomeranged on him as he battles to extricate himself from a war forced on him by Israel, which has resulted in enormous economic and political, not to mention military, losses for the US and Trump. Consequently Israel, in the eyes of many leading political commentators, is now a liability for the US.
How this war was started reveals the dastardly and barbaric mentality of Netanyahu and Trump. The US and Iran were engaged in negotiations, with the mediation of Oman, to resolve their differences, and on 26 February, 2026, the Foreign Minister of Iran stated that a historical agreement with the US was about to be entered into and, the following day, Oman corroborated this announcement. Iran apparently had agreed that its nuclear programme could be brought under the surveillance of the International Atomic Energy Agency. Surprisingly on 28 February, 2026, Israel and the US attacked Iran, Trump saying that it posed a nuclear threat to the US! Oman said it was “dismayed” and the Iranian Foreign Minister said it was a “betrayal”. Obviously, Trump, who is under obligation to the Jewish lobby, which had funded his election campaign, had been drawn into the war. The Epstein files issue may have pushed Trump across the threshold. Iran’s response was calculated and appropriate. Trump says he will obliterate the Iranian civilisation in one night but soon agrees to have negotiations with Iran, in Islamabad.
However, Netanyahu cannot afford an end to the war he started to save his own skin. He goes ahead and drops 100 bombs in 10 minutes on Lebanon, killing 254 civilians, including children. The massacre in Lebanon continues with Israel pushing towards the Litani river in an attempt to annex southern Lebanon. Israel disqualifies itself not only as a reliable ally but also as an honourable member of the world community by having leaders of the calibre of Netanyahu. Israel is fast becoming internationally isolated, according to experts like Professors Robert Pape, John Measheimier, Richard Wolff, Jeffrey Sachs and Yanis Varonfakis. And these experts are of the view that if Israel continues its aggressive approach and expansionist policy, disregarding the historical facts of its origin and the Palestine problem, it will implode and destroy itself.
Israel must face the reality that Iran has emerged stronger after the war and may have control over the Strait of Hormuz and may even force the US out of the region. Israel, under Netanyahu, may not be willing to acknowledge these facts, but the people in the US must realise that it is not in their national interests to have Israel as an indispensable ally. This war is very unpopular in the US not entirely due to the economic impact but the extremely atrocious way it has been prosecuted by Israel and also the equally horrendous threats made by the US against Iran. It is also very unpopular among the US allies who bluntly refused to join or even approve it. Australia, Japan and South Korea, though far removed from the theatre of war, seem to be pretty angry about the whole thing, as they are badly affected by the economic impact of the war. They may be concerned about the brutality of Israel, and the degree of support and approval it gets from the US.
Those who have significantly gained from the war may be Russia who could have a windfall on their oil sales, and China who could quietly weave its diplomatic network throughout the Middle East and watch the decline of US influence in the region. Saudi Arabia and UAE, two countries bombed by Iran, have already started a dialogue with Iran. These developments may hasten the emergence of the new world order, spearheaded by China.
The war, that was started by Netanyahu, with a willing Trump, seems to have backfired on them, with both facing a hostile world and a fast changing geopolitical global situation. Trump’s MAGA project was aimed at quelling the growth of the new world order that had China and Russia at the head. He attempted to hit Russia with sanctions but failed. He tried to curb China with tariffs but failed. Denying oil supplies to China was attempted by kidnapping the Venezuelan President. China’s monopoly on rare earth minerals was a headache to Trump and he proposes to annex Canada and Greenland which have rich deposits of these elements. War on Iran was another opportunity to do a regime change and get control over that country and its oil. He threatened to wipe out Iran saying that “the civilization would die tomorrow night”, only a psychopathic megalomaniac could make such utterances , not a president of the US. Fortunately, the changing world order would not allow Trump to achieve any of his crazy goals.
Netanyahu inadvertently may have hastened his own downfall by starting a war without realising that the global geopolitics have changed and he cannot have his way even with the full backing of Trump. Both Israel and the US need a regime change if the world is to have peace.
by N. A. de S. Amaratunga

Heat Index at Caution Level in the Northern, North-central, North-western, Western, Sabaragamuwa, Eastern and Southern provinces and in Monaragala district.

Dasun Shanaka handed one-year PSL ban

Nahid, Tanzid help Bangladesh level New Zealand series

Five UAE cricketers given citizenship through naturalisation

Moni, Sharmin help Bangladesh register maiden ODI win against Sri Lanka

Advisory for Severe Lightning issued for all provinces of Sri Lanka

‘Dates have the highest sugar content to fight Coronavirus’

Sunday Island 27 December – Headlines

#SundayIsland 17th December – Headlines

Sunday Island – 28th March

Sunday Island Headlines – 21 March

Sunday Island – 21st February – Headlines
-

 News5 days ago
News5 days agoPNS TAIMUR & ASLAT set sail from Colombo
-

 Business3 days ago
Business3 days agoHarnessing nature’s wisdom: Experts highlight “Resist–Align” path to resilience
-

 News3 days ago
News3 days agoGratiaen Trust announces longlist for the 33rd Annual Gratiaen Prize
-

 Latest News7 days ago
Latest News7 days ago“I extend my heartfelt wishes to all Sri Lankans for a peaceful and joyous Sinhala and Tamil New Year!” – President
-

 News2 days ago
News2 days agoFrom Nuwara Eliya to Dubai: Isha Holdings markets Agri products abroad
-

 News3 days ago
News3 days agoHeroin haul transported on 50-million-rupee contract
-

 Latest News4 days ago
Latest News4 days agoSingapore Zoo’s first Sri Lankan leopard cubs make their public debut
-

 Latest News7 days ago
Latest News7 days agoUS blockade of Iran would worsen global energy crisis, analysts say