Features
Giving life to days

UHKDU Palliative Care Services Unit
By Sajitha Prematunge
Fifty six year-old Somalatha was diagnosed with end stage cancer and was already bedridden by the time she was admitted to hospital. With proper care she was able to walk again and was looking forward to making a secure future for her children. But tragedy struck Somalatha’s family again. After her husband suddenly died of a stroke, she was forced to fend for herself. Soon after her condition worsened. Unfortunately Somalatha didn’t live to see her kids receive scholarships with the help of the dedicated University Hospital, Kotelawala Defence University staff, who cared for her.
Although her name is fictitious her predicament is all too real and thousands like her die annually without vital palliative care they are denied just because they couldn’t afford it. It is true that the Sri Lankan healthcare system is one of the best in the world, in that it is almost exclusively free of charge. But no system is infallible. It is patients like Somalatha who have to bear the brunt of its shortcomings, falling through the cracks of the Sri Lankan healthcare system.
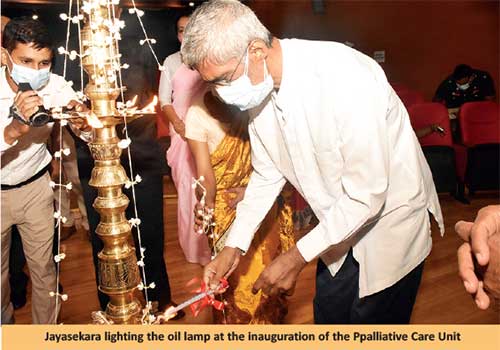
In this light, University Hospital, General Sir John Kotelawala Defence University Palliative Care Services Unit, inaugurate on February 3 should be lauded as a timely intervention, although they had been practising palliative care long before. The UHKDU Palliative Care Services Unit was initiated at a time when repeated attempts to establish such services by various institutions had failed.
Palliative care
 “The simple definition of palliative care is to optimise the quality of life of patients and care givers or loved ones, from the moment the patient is diagnosed with a chronic illness. The definition of ‘chronic’ here has wide implications, ranging from terminal cancer, schizophrenia, chronic neurological diseases, motor neuron disease, stroke to multiple fractures. Any of these conditions require palliative care,” said Consultant Oncologist Dr. Sachini Rasnayake.
“The simple definition of palliative care is to optimise the quality of life of patients and care givers or loved ones, from the moment the patient is diagnosed with a chronic illness. The definition of ‘chronic’ here has wide implications, ranging from terminal cancer, schizophrenia, chronic neurological diseases, motor neuron disease, stroke to multiple fractures. Any of these conditions require palliative care,” said Consultant Oncologist Dr. Sachini Rasnayake.
It is difficult to believe that this personage of slight build heads Palliative Care Services at UHKDU, deftly fielding inquiries of changes to medication, pain management, financial issues and fears of patients, while breaking bad news to patients as gently as possible on an all too regular basis. “The responsibility of the palliative care giver is to uplift lives of the patients physically, psychosocially and spiritually,” said Rasnayake.
Goals
UHKDU Palliative Care Services was established with four main goals in mind. The first of which was to appoint a palliative care team. Rasnayake said that having so many expert consultants from different fields within the UHKDU was an added advantage. “A number of consultants volunteered to provide their services,” said a grateful Rasnayake. She opined that this team spirit was vital in establishing palliative care services. “A team of consultant anaesthetists volunteered to conduct a pain management clinic,” said Rasnayake, who pointed out that pain management is key priority when dealing with any chronic illness. “A group of physicians volunteered to attend to medical issues of palliative care patients. Onco-surgeons and the surgical team looks into the surgical aspect of palliative care.” For example, a Percutaneous Endoscopic Gastrostomy (PEG) tube is surgically inserted into a patient’s stomach through the abdominal wall for feeding purposes. “This is much more desirable than the nasogastric (NG) tube. An NG, inserted through the nose, past the throat, and into the stomach, is very uncomfortable for the patient.”
The team at UHKDU has performed the procedure on multiple long term paralysed patients and patients with throat cancers. “Long term bedridden patients require catheter care and may suffer from urinary incontinence, accidental or involuntary loss of urine; or faecal incontinence, accidental or involuntary loss of faeces or flatus.” Rasnayake explained that indwelling catheters could cause a host of other problems such as urinary track infections. “Genitourinary (GU) surgeons are tasked with addressing such issues.” Rasnayake appreciated the fact that the few oncologists at KDU were able to volunteer for palliative care despite their heavy workload. “Palliative care at UHKDU has no designated Medical Officers. But with much difficulty we were able to secure one nurse. The whole oncology team along with the pharmacists are all experts at palliative care and are wholeheartedly supportive of this initiative.” The rest of the palliative care team consists of a dedicated group of psychiatrists, psychologists and ENT surgeons.
Their second goal is to conduct ongoing medical education programmes. She explained that the team, including the supporting staff had undergone training. “By 2022 we hope that the whole hospital staff would be trained in palliative care,” said Rasnayake hopefully. “It’s vital that everyone undergoes training, since every service accompanies a component of palliative care.” Rasnayake informed that virtual teaching clips were used to train and online assessments used to ascertain the success of candidates, validated through a certification process. “If there is one thing we learned from the COVID-19 pandemic, it’s how pragmatic and applicable virtual training is. For example training a whole staff at the same time would mean that they would have to expend vital work hours. But with virtual training clips the potential care-givers can learn at their own pace.” UHKDU, Executive Director and Senior Consultant Psychiatrist, Dr Jayan Mendis was the first to identify the crying need for a palliative care facility within the University Hospital. Mendis reiterated the significance of such an initiative, pointing out that the training students receive at the facility will be crucial.
The third goal is to provide palliative care home visits. Rasnayake explained that such a service would be beneficial to bedridden patients who experience financial constraints. “Unfortunately we still don’t have a free a

mbulance service.” Rasnayake said that while serving in Polonnaruwa the Cyril Dharmawardana Foundation provided an ambulance service free of charge, which facilitated Rasnayake’s travel to distant parts of the country so she could provide palliative care services to patients who could not afford to travel. “With home visits we can address issues such as constipation, administer IV drips, train care givers and optimise the condition of the patient’s accommodation, including lighting and ventilation.”
The fourth goal is to establish a palliative care hospice. “Palliative Care Unit, Karapitiya Teaching Hospital, Onco Sergeon Dr. Krishantha Perera has achieved just this,” said Rasnayake. “There isn’t such a hospital in Colombo.” She explained that a hospice would see to the psychosocial well being of a patient, in a homely environment, providing symptomatic support. Towards achieving their last goal KDU Vice Chancellor Major General Milinda Peiris has announced his agreement to allocate 10 such rooms from the KDU hotel, to extend this facility to short term palliative care patients. “For the first time in Sri Lankan health tourism, UHKDU has introduced the hospital hotel concept,” said Peiris. “Moreover, in an emergency the patient can be transferred to the hospital in less than five minutes.”
Rasnayake informed that a host of other services concerning palliative care is provided in-house by physiotherapists, psychologists and social workers. Providing radiation therapy at the palliative care facility is also in the works. “But to establish such services and facilities we must have the man power and resources,” Rasnayake pointed out. Rasnayake said that manpower, resources and understanding are integral to palliative care, aspects Sri Lanka is lagging behind in, compared to developed countries. “Unfortunately this has not been well communicated to the community. Most don’t know how they can provide such services,” said Rasnayake. She explained that this is the greatest difference between a hospital and a hospice. “At a hospice you can offer your services, clean and wash patients, subject to supervision, and even entertain them. In a hospital there are rules and regulations that prevents this.”
“One doesn’t have to be medically proficient to practise palliative care. Many who’ve had fallen on hard times in their lives later want to help others through such times,” said Oncology Department, Research Assistant, Dr. Sandini Liyanage. Liyanage and her ilk are stuck between a rock and a hard place. “We want to help, but there’s only so much we can do. We can only treat the patient, with chemotherapy or radiotherapy. But a lot more goes on in the patients’ lives. A terminal illness entails a host of psychosocial issues.” For example, Liyanage explained that, from the moment someone is diagnose with stage four cancer, they’ll invariably start to worry about everything from money, treatment to how to educate their children. “They will mentally fall apart.” Liyanage who is volunteering for palliative care service said that the services are available to any patient, although most who currently receive services are oncology patients. “It’s not just about treating the cancer. The families are also devastated. Cancer takes not only lives but a lot of other things from the family the patient leaves behind.”
Socio-economic constraints
As medical officers of palliative care those like Liyanage are able to build a complete picture about the socio-economic background of a patient by studying their history. She pointed out that most of the patients who require palliative care services are of lower socio-economic backgrounds, who were struggling to make ends meet when the illness in question exacerbated the situation.
“That’s why communication is vital. Palliative care strives to provide a patient-friendly environment,” said nurse Yashmi Kaushalya. Oncology Department nurse, the only such working full time for the Palliative Care unit, Kaushalya is a far cry from the average nurse. With a temperament befitting palliative care, Kaushalya’s calm and measured speech will no doubt assuage her patients. “As nurses we are required to communicate with patients and family members.” Palliative care nurses must be privy to psychological, physical, socio-economic problems of patients. She opined that palliative care is instrumental in caring for patients who have little family backing.
As a nurse new to palliative care, Kaushalya has not broken bad news to a patient’s family yet, for which she would accompany Rasnayake tomorrow. “It can’t be easy breaking bad news,” admitted Kaushalya. “In fact, our services have a lot more to do with caring for patients psychologically than physically,” said Kaushalya. “This is what makes palliative care nurses different from the average nurse.”
“When the patient does not have money to buy drugs, palliative care ends then and there. Although palliative care has been practised for ages, when social and financial capability is curtailed the quality of service drops. This is why social and economical support is vital,” admitted Rasnayake, who had bought drugs for patients out of her own pocket on several occasions. She reiterated that trust and continuous social care services and above all financial support is imperative for maintaining sustainable palliative care.
Rasnayake is positive that money will not be an obstacle for the continuity of the programme. Cancer Care Association founder and Chairman of the National Authority on Tobacco and Alcohol, Dr. Samadhi Rajapaksa provides much needed support, while Indira Caner Trust Director Dr. Lanka Dissanayake and Cancer Society President Anuja Karunaratne have pledged support for the programme. Rasnayake emphasised the significance of establishing a palliative care trust and a governing body to coordinate funds and all stakeholders, to ensure continued support for patients. Rasnayake appreciated the support of senior journalist and former diplomat late Bandula Jayasekara in making the programme a success.
Rasnayake readily admits that Oncology Department Head, Senior Oncologist Dr. Jayantha Balawardhane is the driving force behind the programme. Balawardhane explained that the main objectives of palliative care is to relieve and comfort patients. He pointed out that palliative care can be conducted in the ward, acute care hospital, palliative care unit or hospice, hostel, nursing home, elders home or one’s own home. “Place is immaterial when it comes to palliative care.” Balawardhane emphasized that pain relief is an integral part of palliative care. “Relieving pain is half the battle in palliative care.” Other discomforts such as bedsores, loss of bladder and bowel control adds insult to injury.
Psychosocial issues
Psychosocial issues such as sense of abandonment, anger, frustration and resentment exacerbate the psychological condition  of the patient. “Patients maybe embittered, therefore we must address such psychosocial issues with care,” reiterated Balawardhane. Social abandonment, resulting from stigma, due to myths such as cancer is contagious or associating those undergoing chemo or radiation therapy could adversely affect others, and busy schedules that prevent loved ones from visiting are among the major social issues faced by palliative care patients. “Cosmetic mutilation is also a major issue,” pointed out Balawardhane. Treatment results in hair loss, palloring of skin and weight loss and this contributes to patients becoming social outcasts.
of the patient. “Patients maybe embittered, therefore we must address such psychosocial issues with care,” reiterated Balawardhane. Social abandonment, resulting from stigma, due to myths such as cancer is contagious or associating those undergoing chemo or radiation therapy could adversely affect others, and busy schedules that prevent loved ones from visiting are among the major social issues faced by palliative care patients. “Cosmetic mutilation is also a major issue,” pointed out Balawardhane. Treatment results in hair loss, palloring of skin and weight loss and this contributes to patients becoming social outcasts.
“Palliative care must also respect cultural differences and religious inclinations. For example, one who may believe in reincarnation may attempt to weigh one’s merits and demerits, contemplating on where he or she would be reborn. All this contribute to the suffering of the patient,” said Balawardhane. Quoting from American neurosurgeon, pathologist and writer, Harvey Cushing, Balawardhane said that, “‘A physician is obligated to consider more than a diseased organ, more even than the whole man – he must view the man in his world’, meaning that palliative care is holistic care. Most importantly it should be patient centred, family centred.” Palliative care should be comprehensive, leaving no stone unturned, continuous and proactive, delivered by a coordinated team and subject to regular review.”
The palliative care team consists of nurse, dietician, pharmacist, occupational therapist, paramedical aid, General Practitioner, bereavement support worker, social worker, councillor, domestic care provider and even the funeral director plays a vital role in the team. Palliative care is a support system that facilitates an active lifestyle for as long as medically possible. “This requires a lot of distractions such as games like carom, card or scrabble, listening to music or watching TV.” Palliative care practitioners use their clinical expertise and judgement to anticipate problems and treat them proactively before they manifest. “Integration of psychological, emotional, social and spiritual aspects of care between patient, family and caregivers is imperative to the functioning of the palliative care process,” emphasised Balawardhane.
Palliative care trains the patient to regard dying as a normal process, by improving the quality of life for the remainder, explained Balawardhane. “Quality is subjective, it differs from person to person.” he explained that the care provider must not enforce what he or she assumes as ‘quality’ on the patient and in stead must cater to patient demand. Palliative care promotes a degree of acceptance by the patient and immediate family, regarding the final outcome and assists the patient in the decision-making process that would result in a peaceful and dignified demise. Bereavement support helps loved ones to accept loss and does not abruptly stop with the demise of patient under palliative care. “The objective is to give life to days, whatever the remaining number of days, and not give days to life.”







For a considerable length of time in the past, the global war on cancer relied on a strategy similar to carpet-bombing or shooting from the hip in a wider circle. Traditional chemotherapy, while lifesaving for millions, has always been a blunt and aimless instrument. It floods the body with medications that attack any cell that divides rapidly, and because cancer cells divide ever so speedily, they too are destroyed. However, those chemotherapy drugs also attack the healthy multiplying cells all over the body, including those in the hair follicles, stomach, intestinal lining, and bone marrow. It was a kind of an all-encompassing blunderbuss approach. The end result is the all-too-familiar gauntlet of severe nausea, loss of appetite, hair loss, bone marrow depression, as well as profound exhaustion.
But a quiet and profound revolution has been unfolding in the corridors of oncology. Western medicine is rapidly shifting away from this one-size-fits-all assault. Instead, we are entering the era of precision oncology: a paradigm shift where treatments are tailor-made to target the specific genetic and molecular aberrations lurking inside a tumour. In a telling analogy, modern cancer therapy is deploying snipers instead of grenades or carpet bombs. Nowhere is this revolution more visible or more successful than in the fight against blood cancers and lymphomas.
Decoding the Enemy: What are Antigens and Tumour Markers?
To understand how this new generation of medicine works, we have to look at the microscopic histological landscape of a cancer cell. Every cell in the body is covered in unique surface proteins, which act like microscopic identification badges. The immune system scans these badges to differentiate between one’s own healthy tissue and foreign invaders like bacteria or viruses. When any such protein triggers an immune response, it is called an antigen.
When a normal cell transforms or mutates into a cancerous one, its identification badges change. It begins to overexpress certain proteins, display mutated or altered versions of them, or throw out chemical distress signals. Scientists refer to these telltale chemical signatures as tumour markers.
In the past, two patients with the same type of lymphoma would receive exactly the same chemotherapy regimen because their tumour cells looked identical under a standard microscope. Today, molecular testing can reveal that Patient X’s tumour cells are covered in a specific antigen, while Patient Y’s tumour even lacks it entirely. Though the cancer has the same name, the underlying biology is completely different. By identifying these distinct tumour markers, doctors can now select a drug designed specifically to latch onto that exact marker, leaving the neighbouring healthy cells virtually untouched. It is akin even to modern drone technology.
The Breakthrough in Blood Cancers and Lymphomas
While precision medicine is making waves across all of oncology, its most dramatic victories have been won in haematological malignancies; the cancers of the blood, bone marrow, and lymph nodes. Blood cancers are uniquely suited for targeted therapies. Unlike a solid tumour in the lung or colon, which can be a chaotic, structurally complex mass of many different cell types, blood cancers often stem from a single, rogue line of immune cells circulating through the body. This makes it easier for scientists to isolate the specific “glitch” or antigen common to the entire cancerous population and then attack it specifically.
The Story of Rituximab: The First Smart Bomb
Consider the case of a Non-Hodgkin Lymphoma, a cancer of the lymphatic system. A vast majority of these lymphomas arise from cancerous B-cells (a type of lymphocytic white blood cell). Scientists discovered that these malignant cells almost universally carry a specific surface antigen called Cluster of Differentiation or Cluster of Designation, universally known by the abbreviation CD20.
This discovery led to the creation of the medication Rituximab, one of the earliest and most successful monoclonal antibodies. Monoclonal antibodies are laboratory-produced molecules engineered to mimic the body’s natural immune system. They act like guided missiles, designed to seek out and bind to specific proteins or foreign invaders to block disease processes, stop inflammation, or flag infected cells for natural destruction. Engineered in a lab, Rituximab behaves like a heat-seeking missile or a drone, designed to seek out and bind exclusively to the CD20 antigen.
Once it locks onto the cancer cell, it does two things: It delivers a direct blow to the cell’s internal machinery and simultaneously acts as a neon sign, screaming to the patient’s own immune system: “Come and destroy this specific cell.” The introduction of targeted therapies like Rituximab radically transformed the prognosis for lymphoma patients, turning what was once a highly fatal diagnosis into a highly manageable, often curable condition.
Turning the Patient’s Body into the Medicine: CAR-T Cell Therapy
If monoclonal antibodies are smart bombs, the latest frontier in tailored treatment is akin to training an elite, personalised army. CAR-T Cell Therapy (Chimeric Antigen Receptor T-cell therapy) is a highly specialised form of immunotherapy that genetically modifies a patient’s own white blood cells (T-cells) to seek out and destroy cancer cells. The use of the term Chimeric ” indicates a tissue with two or more genetically distinct populations of cells. This is the essence of CAR-T cell therapy, a living drug tailored not just to a type of cancer, but to the individual patient.
The process sounds like science fiction, but it is saving lives today. A patient’s white blood cells (T-cells, the foot soldiers of the immune system) are harvested from their blood. These cells are then genetically re-engineered in a specialised laboratory by using a harmless virus to insert a new gene into these T-cells. This gene instructs the cells to grow a specialised receptor on their surface called a Chimeric Antigen Receptor (CAR). This receptor is custom-built to recognise the exact antigen on the patient’s cancer cells (such as CD19 in acute leukaemia). Then these newly armed “super-cells” are grown by the millions in a laboratory and infused back into the patient.
Once back inside the body, these living weapons hunt down the cancer cells with astonishingly targeted precision. As they are the patient’s own cells, they can persist in the body for years, acting as a vigilant, microscopic security guard against any relapse.
The Benefits: Better Results, Kinder Side-Effects
The most immediate benefit of tailored therapy for the average patient is the reduction in collateral damage. Because these drugs are engineered to ignore cells that do not bear the target antigen, the devastating side effects of traditional chemotherapy are heavily mitigated. Patients generally do not lose their hair, and the severe, debilitating nausea that once defined the cancer experience is significantly lessened.
Furthermore, these treatments work where chemotherapy fails. Cancer cells are notoriously cunning; they often evolve mechanisms to pump chemotherapy drugs out of their system or repair the DNA damage caused by standard drugs. Targeted therapies bypass these defence mechanisms by attacking the cell’s unique structural vulnerabilities or cutting off the specific growth signals the tumour needs to survive.
Challenges on the New Frontier
Despite the immense promise, the transition to fully tailored cancer care is not without its hurdles. At these initial times, these therapies are not panaceas for all ills.
Cancer cells are highly unstable and prone to frequent mutations. A drug may successfully eliminate 99% of tumour cells bearing a specific antigen, but the remaining 1% might mutate, stop producing that antigen, and begin to multiply. This is known as “antigen escape,” leading to drug resistance. To counter this, researchers are now developing therapies that target multiple different markers simultaneously, trapping the cancer in a molecular crossfire.
Tailored treatments are marvels of modern biotechnology, but they are incredibly complex and expensive to manufacture. Designing a unique cellular therapy for a single individual requires highly sophisticated infrastructure, specialised laboratories, and pristine quality control. Lowering the cost of production so these life-saving treatments are accessible to patients worldwide remains one of the greatest challenges of 21st-century medicine.
A targeted drug is only useful if you know exactly what you are targeting. This requires patients to undergo advanced genetic sequencing and biomarker testing at the time of diagnosis. Integrating these sophisticated diagnostic tools into routine medical care globally is essential if we are to realise the full potential of precision oncology.
The Road Ahead: A Future Without “Cancer” perhaps!!!
It is not wishful thinking. We are rapidly approaching a future where the word “cancer” will no longer be treated as a single, terrifying megalith. Instead, a patient’s diagnosis will be defined by its specific molecular profile: a unique combination of antigens, genetic mutations, and tumour markers. The swing towards tailored treatments in Western medicine represents more than just a technological advancement. It perhaps represents a philosophical shift. We are no longer treating the disease in isolation; we are treating the specific, unique manifestation of that disease within an individual person.
While there is still a long winding road ahead to conquer drug resistance and ensure equitable access to these therapies, the future trajectory is quite clear. The era of carpet-bombing is drawing to a close. The age of precision medicine has arrived, bringing with it unprecedented hope, gentler recoveries, and a brighter dawn, especially for cancer patients around the world. Hail Personalised Medicine; Vivat Medicina Ad Personam.
by Dr B. J. C. Perera
MBBS(Cey), DCH(Cey), DCH(Eng), MD(Paediatrics),
MRCP(UK), FRCP(Edin), FRCP(Lond), FRCPCH(UK), FSLCPaed, FCCP, Hony. FRCPCH(UK), Hony. FCGP(SL)
Specialist Consultant Paediatrician and Honorary Senior Fellow,
Postgraduate Institute of Medicine, University of Colombo, Sri Lanka.
An independent freelance correspondent.

The Pilot
Francis Gary Powers was born in Jenkins, Kentucky on August 17, 1929, the only son in a family of six children. His father, Oliver Powers, was a coal miner struggling through the Depression years. At the age of 14, Francis took a joy ride in a light aircraft at a country fair in exchange for $2.50. Immediately bitten by the ‘flying bug’, he decided that he wanted to be a pilot someday, although his father wanted him to be a doctor. By then World War II was on, and Francis planned to join the US Navy after completing high school graduation. But when the time came, the war had ended and Francis missed that opportunity.
However, at his father’s suggestion he enrolled at the Milligan College in Tennessee. In his senior year there he applied to become a US Air Force cadet, and was selected, with the stipulation that only after graduating from Milligan would he be allowed to sign his papers for entry as a cadet. As the Korean war had begun, Powers’ father preferred him to return home after graduation and wait for his draft notice for war service. Powers complied, but after two months he applied again to the US Air Force, was selected and enlisted.
His initial training was in skills other than flying, mainly photography. Eventually, in November 1951 he joined the flight school and commenced training on a North American T-6 Texan. Six months later, he began learning to fly jet aircraft, with Powers desperately wanting to participate in combat over Korea. But he was stricken with appendicitis and missed out on the action.
Subsequently, in October 1953 he was sent to New Mexico to train on aerial nuclear bombardment missions at the Watertown airbase, believed to be the birthplace of the Central Intelligence Agency (CIA) and later dubbed ‘Area 51’. Meanwhile, Powers was planning to enter ‘civvy street’ as an airline pilot after completing his period of military service. However, he discovered that by the time of his release from the USAF he would be overage for selection by the airlines, so now with a wife to support, Powers decided to renew his tour of duty with the USAF.
In late 1955 Francis was approached by the CIA to fly a specialised type of intelligence-gathering airplane. Manufactured by Lockheed and developed in Area 51, the aircraft was dubbed the ‘Utilities 2’ (‘U-2’ for short). However, he would work ostensibly as a civilian pilot for the CIA. While regular pilots in the USAF were earning $400 per month, this job came with a monthly salary of somewhere between $1,500 and $2,000, with the pilot based overseas basing. For Powers it was an attractive proposition, not least because it was an opportunity to do something patriotic in a new type of aircraft.
As for operations in the U-2, because flights were conducted close to outer space, pilots could see the curvature of the earth, and had to wear a proper space suit, like astronauts. As sunlight was reflected from below, at those altitudes when pilots looked up all they saw was darkness. Once a pilot was cocooned inside his partial-pressure space suit, like an astronaut’s, his full-pressurized helmet was ‘hermetically sealed’ to the extent that he couldn’t even scratch his nose! And if the suit failed or was damaged, the pilot’s blood would literally boil.
The Aircraft
After WWII, with the advent of the ‘Cold War’, the USSR put up their ‘Iron Curtain’. US President Dwight Eisenhower realised it was imperative for the US to look over the other side of that invisible wall to see what was happening there. By then the Soviets had also acquired nuclear capability. While the USAF had aircraft such as the Boeing B-52 Stratofortress with sufficient range and capability for intelligence-gathering, unfortunately the bombers could operate only at lower altitudes, within easy reach of Soviet missiles and fighter jet aircraft. What the USAF needed was an aircraft which could fly above 70,000 ft for at least ten hours at a time.
After evaluating many options, Lockheed applied the resources of its legendary top-secret ‘Skunk Works’ development programme to design and produce a single-engine aircraft with a 105 ft wingspan (measured from wing tip to wing tip) capable of meeting the USAF’s latest requirements. Working under the direction of Lockheed’s equally renowned designer, Kelly Johnson, the team built a prototype in only eight months by combining the fuselage of a Lockheed F-104 Starfighter (a type labelled by pilots as the ‘widow maker’) with newly-designed ultra-long wings. As much weight as possible was saved by providing the barest minimum of equipment, without any armaments, except for the high-resolution camera. Even the canopy enclosing the pressurised cockpit wasn’t fitted with an electric motor to open and shut it, as that would have added to the airplane’s weight. With the ‘empty’ aircraft weighing much less than it otherwise would have, a spin-off benefit was greater fuel efficiency by carrying the maximum amount of fuel, in integral tanks in the wings and nose, for the long surveillance flights for which the U-2 was primarily designed.
The U-2’s landing gear (undercarriage) comprised two main wheels mounted in tandem at the nose and tail along the longitudinal axis, not unlike wheels on a bicycle. For stability during taxiing and takeoff, two smaller wheels were attached to outriggers at each wingtip. These wheels were designed to fall away as the aircraft lifted off, then retrieved for reuse by a ground crew. However, the absence of the outrigger, or ‘pogo’, wheels made the U-2 difficult to land and roll along the runway at the end of a mission.
The spy-plane’s long wings were so efficient that they produced lift even with the General Electric turbofan engine on idle power close to the ground (with the aircraft flying in what is called ‘ground effect’), while the landing gear, flaps and spoilers helped to create drag to slow the aircraft down. During the landing process another U-2 pilot in a chase car (called the ‘mobile’) followed the aircraft when it was directly above the runway, giving the pilot of the landing U-2 guidance in flying parallel close to the ground, before he induced an aerodynamic stall to touchdown by raising the nose. Performance-wise the aircraft could take off within less than 1,000 ft of runway and climb quickly to the planned very high altitude.
Pilots called the U-2 the ‘Dragon Lady’. It was relatively slow with a cruise speed of Mach 0.7, i.e. 70% the prevalent speed of sound. (Today’s big commercial jets fly at speeds between Mach 0.80 and 0.85.) For the more technically minded, the difference between the low-speed stall and high-speed stall was only eight knots. (‘Stall’ in this instance refers to an aerodynamic stall, whereby the lift-generating airflow over the wings deteriorates causing the airplane to descend. It is distinct from an engine stopping, or ‘stalling’.) Consequently, U-2 pilots had to be very gentle with the controls.
Another characteristic of the U-2 is that it flew very close to what is known as ‘Coffin Corner’ at high altitude. To explain that term and phenomenon, an aircraft remains airborne as the force of lift, produced by airflow over its wings, is equal to the airplane’s weight, while the thrust generated by its engines is equal to aerodynamic drag, or resistance. Lift is also proportional to the density of the air through which the aircraft flies. As an aircraft reaches higher altitudes, air density reduces, and consequently the ‘lifting power’ deteriorates too. If nothing is done to stabilize the aircraft it will begin descending or literally fall out of the sky from lack of lift. Therefore, to maintain the value of the lift component and keep the airplane aloft at those ultra-high altitudes, the aircraft must fly faster with the engine(s) at full throttle.
Additionally, as the aircraft approaches the speed of sound, the air flowing over the top of the wing, which is usually curved to generate lift, tends to move faster than the speed of sound and creates a shock wave. However, the speed of sound reduces with Absolute Temperature, therefore the aircraft reaches the sound barrier earlier at a lower speed at high altitude. Again, the aircraft could fall out of the sky by going too fast. Those are the problems that must be reckoned with when flying at high altitudes, hence the expression ‘Coffin Corner’.
The Mission
On May 1, 1960 Francis Gary Powers was assigned to a mission code-named ‘Operation Grand Slam’, to fly from Peshawar, Pakistan to Bodø in Norway, taking photos along the way. As the USSR was busy celebrating May Day in its usual grandiose manner, CIA planners thought it would be a good opportunity to launch the covert photo reconnaissance flight on that day. Ater lining up for takeoff, Powers had to await authorisation from Washington. The ‘Go Signal’ would be received on High Frequency (HF) Radio relayed via Turkey by Morse code.
Departing Peshawar at 0626 hours, Powers climbed quickly through 66,000 ft, then clicked his microphone twice to indicate that he was well and operations were normal. That was the last anyone monitoring the flight heard from him. Reaching 70,000 ft, the U-2 entered USSR airspace from over Lake Van in Northeastern Turkey. But the Soviets were monitoring his flight almost from departure point and waiting for him.
As it happened, there had been a similar U-2 flight the day before. But as none of the Russian fighter jets or missiles could reach 70,000 ft, complacency had set in among the Americans. This morning however, when Powers was passing Lake Van, an explosion occurred behind his U2. Three missiles had been launched by the USSR, one of which struck one of their own fighter aircraft in error, with another going astray. But the missile that detonated in close proximity to Powers’ U-2 was more successful. As the spy-plane was relatively ‘flimsy’ for the purpose of saving weight, the explosion’s shock wave was strong enough to tip the aircraft over in a nose-down attitude. The resulting g-forces pushed Gary Powers up in his seat toward the cockpit canopy and out of reach of the self-destructive switch designed to destroy the on-board camera and film. Still in control of the airplane, Powers descended to 30,000 ft but found that he was now too low to eject. Then a second missile struck the aircraft, throwing him out of the cockpit. His parachute deployed automatically and he landed on a Soviet community farm where he was soon apprehended and handed over to the authorities (KGB). Powers did not, however, use the lethal poison-laced pin, hidden in a coin he carried, to kill himself.
Meanwhile, the CIA realised that one of its U-2 spy-planes had gone missing, so they put out a standard cover story from their files saying that it was an unarmed NASA weather observation aircraft that had been shot down. They claimed that the airplane had suffered an oxygen system problem, with the resulting hypoxia possibly disorientating the pilot. The CIA added that almost certainly the pilot would not have survived, and that was the version announced to the world by President Eisenhower.
However, it wasn’t until May 7 when Soviet Prime Minister Nikita Khruschev announced that an American U-2 had been shot down and its pilot captured. Finally, Eisenhower was forced to admit on May 11 that he had lied, and that he had authorised the spy flights over the USSR.
With the Cold War showing signs of thawing slightly (although the Cuban missile crisis was still two years in the future), a high-level summit meeting had already been planned for May 16 between the US, USSR, Great Britain, and France in Paris. The other Communist nations were not pleased with Khrushchev for agreeing to participate. But the U-2 ‘incident’ on May Day now provided him with a convenient excuse not to attend that highly anticipated meeting. Eventually though, he only met French President Charles de Gaulle and British Prime Minister Harold Macmillan individually, then withdrew from the summit in a huff.
Later, on August 31, 1960 – Francis Gary Powers’ 31st birthday – a ‘show trial’ began at the Hall of Columns (Dom Soyuzov) in Moscow. The pilot’s family was present too. But the verdict was preconceived. Although Powers was expected to be executed, as a spy, he was sentenced to ten years’ imprisonment, with a 100 rubles per month of pocket money and permitted to send one letter home each month. But after serving 21 months, on February 10, 1962 Powers was exchanged for a Soviet intelligence officer named Rudolf Abel (born Vilyam Fisher), who had been convicted on espionage charges and incarcerated on a 30-year sentence at the Atlanta Federal Penitentiary in Georgia, USA.
The much-publicised, almost stage-managed exchange took place at the Glienicke Bridge linking West Berlin to East Germany, and later formed the subject of the Steven Spielberg movie ‘Bridge of Spies’ starring Tom Hanks. Significantly, by the time of the prisoner exchange, CIA chief Allen W. Dulles (brother of John Foster Dulles, the former US Secretary of State under President Eisenhower) had been forced to resign over the Bay of Pigs debacle in Cuba and other perceived strategic failures.
Although, after extensive series debriefings the CIA remained ostensibly pleased with Powers’ actions while in captivity in the USSR, President John F. Kennedy cancelled a formal reception to celebrate his return to the USA. Even Powers’ private writings, in the form of a diary he kept during captivity in the USSR, were suppressed by the CIA. However, they were released many years later in the book titled ‘Letters from a Soviet Prison’.
On March 6, 1962, Powers, who had been awarded the CIA Intelligence Star on his return from captivity, fronted an Armed Services Senate Committee who wanted to ensure that he hadn’t divulged state secrets to the Soviet Union. At the end of the sessions the Senate Committee members were so pleased with his conduct whilst in Soviet captivity, they gave him a standing ovation.
Although the media at that time was making things uncomfortable for Powers, he received the back pay that had accrued while he was out of the country, and he resumed flying but as a civilian U-2 test pilot for Lockheed. Over-flights of the USSR were suspended, but surveillance missions continued over countries such as Vietnam, Cuba and Indonesia. Today the U-2 still flies, mainly on weather and communications missions.
Much later, Francis Gary Powers joined Los Angeles TV station KNBC as a helicopter pilot on traffic-reporting duties. But on August 1, 1977, the Bell JetRanger Powers was flying whilst filming brush fires in Santa Barbara County, ran out of fuel and crashed over the San Fernando Valley, killing him and cameraman George Spears.
Frances Gary Powers was only 47 years old at the time of his death. Dick Spangler, President of the Radio and Television News Association of Southern California, lobbied to have Powers buried at Arlington National Cemetery. The request was duly granted by President Jimmy Carter on the basis of Powers having been awarded the CIA Intelligence Star (equivalent to a military Silver Star) for his service as a CIA spy-plane pilot.
Posthumous Awards received by Capt. Francis Gary Powers (in 2000 & 2012):
· Silver Star: Awarded by the US Air Force in 2012 for valor and exceptional loyalty while being held captive.
· Distinguished Flying Cross:
Awarded for actions during his flights.
· Prisoner of War Medal:
Awarded in 2000 for his time imprisoned in the Soviet Union.
· CIA Director’s Award:
Given for extreme fidelity and courage.
· National Defense Service Medal:
Awarded by the Department of Defense.
God Bless America and no one else!
BY GUWAN SEEYA
Tales of Mystery and Suspense 5
When the journalist is found murdered on the Heath, near the house, Bigge realizes what has happened, a conclusion that the reader too might well have come to, except the rationale for what had happened continues obscure until the end. For there are fascinating twists with regard to the motive, and other twists with regard to the odd motivations of the other characters.
My visit to Australia last year was immensely productive, not only because it was the precursor to a cruise on the Pacific, but also because I was given several books by friends there. Apart from those Robert Scoble gave me, I got two thrillers for the cruise from Peter Rowe, who had been High Commissioner here at the turn of the century, and a very good friend since.
A queer case
He gave me two very different thrillers for the cruise, both of which I managed to finish while on board. The first I read was A Queer Case by Robert Holtom, the first in a series still to be developed about a gay bank clerk, Selby Bigge, who spends much of his free time searching for sex, and also looking for a lover. The novel is set in the period soon after the First World War, when Bigge has to be constantly on the alert to avoid arrest.
Robert
The novel opens with him on Hampstead Heath, the haunt of gay adventurers in those days and I believe even now, along with someone who enjoyed casual sex with him but was not prepared for more, unlike Bigge. When their assignment has to be abandoned, he comes across an Oxford acquaintance whom he had once kissed on a bench there, though nothing further had developed. He feels this may be the lover he seeks, and is thrilled when Patrick tells him how much he hates his step-mother, who he thinks is a gold digger, and asks him to find out more about her.
Patrick invites him to the Ritz to meet his father, Sir Lionel Duker, and his second wife Lucinda. There is a scene there when they are confronted by a journalist who it seems hated Lucinda since she had originally married the man he was in love with. He had persecuted the pair until they were divorced, after which, the man having left the country, Lucinda married Sir Lionel.
Bigge visits the journalist, whom in his relentless search for sex he rather fancies, but the man rejects his advance, and does not seem especially knowledgeable about the gay world, which makes Bigge wonder. He then goes to the Duker mansion near Hampstead Heath, for Sir Lionel’s birthday party, and meets a strange collection of guests including a lady crime novelist who believes she is much better than Agatha Christie and her niece, a lesbian who turns out to be engaged to Patrick.
The journalist turns up after the ladies have left, and Sir Lionel has retired, as has a drunken colonel. Though the journalist is thrown out and flees into the night, Bigge after vainly pursuing him and getting back to the house finds Lucinda has been strangled. Patrick had been locked in the cloakroom, the key of which had vanished earlier in the evening.
The immediate assumption of the police who are called in, as well as everyone else, is that the journalist had slipped into the house and killed Lucinda, but this is not certain and Bigge feels the police have their suspicions about him, too, his nervousness increased by the knowledge that in pursuing their inquiries they will find out about his sexuality. His fear is exacerbated when they turn up at his lodgings; the pick up was with at the beginning of the novel had dropped in for a quickie, and had to hide in his bedroom. Holtom creates much suspense in this very odd situation, before the police finally leave.
When the journalist is found murdered on the Heath, near the house, Bigge realizes what has happened, a conclusion that the reader too might well have come to, except the rationale for what had happened continues obscure until the end. For there are fascinating twists with regard to the motive, and other twists with regard to the odd motivations of the other characters.
In the end, it is the lesbian fiancé who becomes Bigge’s good friend, not Patrick, who they both realize is riddled with guilt about his sexuality. I had thought she would become his amanuensis, but it seems that he acquires an aristocratic male sidekick for his second case, in a book that is due to be published soon.

Wife, counsel seek regular access to ex-Spy Chief Sallay held under President’s detention order

CIABOC summons Yoshitha over his participation in British Navy training programme

Communist Party condemns ill-treatment of Sallay, calls for review of PTA

Justice Minister responds to social media claims he represented Easter Sunday ringleader

Several SLTB Depots suffer losses due to their remote locations

Three Lankans among seven suspects arrested in Kuwait for alleged drug links

‘Dates have the highest sugar content to fight Coronavirus’

Sunday Island 27 December – Headlines

#SundayIsland 17th December – Headlines

Sunday Island – 28th March

Sunday Island Headlines – 21 March

Sunday Island – 21st February – Headlines
-

 News5 days ago
News5 days agoWomen’s T20 World Cup 2026 warm-up: Chamari Athapaththu’s 94 helps Sri Lanka beat Pakistan
-

 News6 days ago
News6 days agoAsst. Manager, security officer arrested over Rs 30 mn snatch at Horana PB branch
-

 Editorial4 days ago
Editorial4 days agoProbe Sallay’s complaint
-

 News5 days ago
News5 days agoLankan-Canadian inducted to Toronto Sports Hall of Fame
-
 News2 days ago
News2 days agoLocal firms move millions of dollars overseas for phantom imports: Govt.
-

 Editorial5 days ago
Editorial5 days agoPrez in the dock
-

 Features5 days ago
Features5 days agoEntering MIT for my Ph.D program, coping with harsh Boston winter and breasting the tape
-

 News6 days ago
News6 days agoNo blanket ban on musical performances; only those promoting LTTE